Abstract
Objective: To examine the sociodemographic and clinical profiles of veterans who primarily rely on the US Department of Veterans Affairs (VA) health care system for their care.
Methods: Data were analyzed from a nationally representative sample of 4,069 US military veterans who participated in the National Health and Resilience in Veterans Study in 2019–2020.
Results: Overall, 20.5% of veterans reported using the VA as their primary source of health care. Compared to non-VA users, these veterans were more likely to be younger, unmarried or unpartnered, and black/African American and to have lower household incomes (≤$60,000 annually). They also reported greater cumulative trauma exposure and were more likely to have a history of depression, posttraumatic stress disorder, and chronic medical conditions such as chronic pain, sleep disorders, and respiratory illnesses.
Conclusion: VA health care serves a distinct and vulnerable subgroup of veterans who experience more complex psychiatric and medical needs, as well as greater financial insecurity, compared to non-VA users. These findings underscore the importance of expanding comprehensive, integrated services that address both physical and mental health conditions while accounting for socioeconomic factors to better meet the needs of veterans who rely on VA health care.
Prim Care Companion CNS Disord 2026;28(3):25m04176
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
The Veterans Health Administration (VHA), a branch of the US Department of Veterans Affairs (VA), is the nation’s largest integrated health care system in the United States, providing care, conducting research, and training health care professionals while serving millions of veterans annually.1,2 Established in 1946, the VHA now operates 1,321 health care facilities nationwide, including 172 VA medical centers and 1,138 outpatient clinics.1 Veterans have access to a wide range of services, including primary and urgent care, surgery, pharmacy, mental health, and specialty services.1,3
The VHA offers several key advantages for veterans. First, eligibility requirements are relatively broad, with most veterans eligible for services if they served in the US military for at least 24 continuous months (or were discharged due to service-connected disability or hardship) and received a nondishonorable discharge.4 In recent years, the VHA has expanded efforts to ensure timely access to care for all VA-eligible veterans through outreach initiatives, interdisciplinary collaboration, and enhanced care management services.1,3
Second, the VHA is specifically designed to meet veterans’ unique health care needs. For instance, the VHA offers routine assessments and provides evidence-based treatments for common medical and psychiatric conditions that are prevalent among veterans, including posttraumatic stress disorder (PTSD), major depressive disorder (MDD), traumatic brain injury (TBI), chronic pain, tinnitus, and multimorbidity.4,5 Given that veterans are, on average, older and at greater risk for mental and physical health problems than the general population,6 access to integrated medical and psychiatric care within the VHA is essential.7
Third, the quality of VHA health care is comparable and often superior to that found in community-based systems. A recent systematic review concluded that VHA care is “as good as, or better than, care in the community.” 3(p2186) Several studies have demonstrated that the VHA outperforms other health care systems on a range of clinical and patient-reported outcomes, including quality of care, safety, timeliness, effectiveness, morbidity, and mortality.3,7 VHA care has been linked to lower mortality for stroke and heart failure, reduced readmission rates, and longer lengths of stay compared to VHA-purchased community care.6
Despite these advantages, many veterans do not use the VHA as their primary source of health care. Contributing factors include access to employer-sponsored insurance3 and access issues.8 Although initiatives such as telehealth and patient-aligned care teams have improved access, many veterans remain unaware of available services or face barriers such as stigma (particularly related to mental health care), transportation challenges, and confusion about benefits, enrollment, privacy, and security.2,8 Lack of access to VHA care may lead to fragmented treatment that fails to address co-occurring conditions or to complete disengagement from health care, particularly among vulnerable groups such as older or unhoused veterans.9 Federal initiatives continue to prioritize improvements in the quality and accessibility of VHA care.8
Prior research has found that veterans who use VHA services differ substantially from those who do not. For example, a nationally representative study conducted in 2011 found that primary VHA users had higher rates of lifetime PTSD, trauma, substance use disorder, suicide attempts, and social phobia, as well as current depression, anxiety, and suicidal ideation.7 They also had higher rates of chronic pain, cardiovascular and respiratory conditions, arthritis, and other medical comorbidities, along with greater functional impairment. While the study highlighted important differences between groups, its findings are based on data collected more than a decade ago and may not reflect recent changes in the veteran population or VHA services.
Since 2011, both the veteran population and the VHA health care system have undergone substantial changes. Between 2011 and 2023, the number of US veterans declined by more than 5.6 million. During this period, the proportion of female veterans grew by 3.6%, the proportion of white veterans declined by 10.2%, and the share of veterans over age 75 rose by 5.5%. Meanwhile, the proportion of Vietnam-era veterans decreased by 2.0%, while the proportion of First and Second Gulf War veterans increased by 8.8% and 16.4%, respectively.10 In addition to these demographic changes, VHA service utilization for both mental health and medical care has expanded, with more than 9.1 million veterans enrolled as of March 2024. In the prior year alone, over 400,000 veterans newly enrolled, reflecting a 30% increase.11 Legislative reforms, including the Veterans Choice Program (2014) and the VA Mission Act (2019), have further increased access to both VA and VA-funded community-based care.12 Additional system-wide changes include a shift toward patient-centered, integrated health services, enhanced outreach and case management, and a rapid growth in telemedicine.13,14
Given these demographic shifts and system-level changes in the VHA, updated information on the characteristics of veterans who rely on VHA care versus those who do not is urgently needed to inform service planning and the delivery of equitable, tailored care. To this end, the present study analyzed data from a nationally representative sample of community-dwelling US veterans to estimate the prevalence of primary VHA health care utilization and to compare demographic, psychiatric, substance use, medical, physical, and cognitive characteristics between primary VHA users and nonusers.
METHODS
Sample
Data were analyzed from the National Health and Resilience in Veterans Study (NHRVS), which surveyed a nationally representative sample of 4,069 US veterans.15 Participants included veterans from all service eras, including Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn, Persian Gulf, Vietnam, Korean War, and other conflicts, who completed an anonymous, web-based survey in 2019–2020. The sample was drawn from KnowledgePanel, an online probability-based survey panel of a representative sample of over 50,000 US adults that covers approximately 98% of US households. Panel members were recruited through national random samples, originally by telephone and now almost entirely by postal mail. To permit generalizability of results to the US veteran population, poststratification weights using benchmark distributions of US military veterans from the most contemporaneous Veterans Supplement of the Current Population Survey were applied. Additional details about the NHRVS methodology can be found elsewhere.15 All procedures were approved by the Human Subjects Committee of the VA Connecticut Health Care System, and all participants provided electronic informed consent.
Measures
Veterans responded to an item about their main source of health care (eg, “Is the VA your main source of health care?”) and were defined as “primary VHA users” or “not VHA primary users” based on this item. Veterans also completed assessments that examine a range of sociodemographic (eg, age, race/ethnicity), military (eg, combat status), trauma (eg, adverse childhood experiences [ACEs]), psychiatric (eg, lifetime and current psychiatric disorder, positive screen for PTSD, current suicidal ideation), medical, mental health treatment utilization, and functioning (eg, psychosocial difficulties) variables, which were examined as potential correlates of primary VA utilization as a main source for health care status. Supplementary Table 1 provides a description of these measures.
Data Analysis
Descriptive statistics examined the prevalence of primary VHA health care utilization. Weighted independent sample t-tests and χ2 analyses compared veterans who did and did not utilize the VHA as their primary source of health care. A multivariable binary logistic regression analysis identified characteristics independently associated with primary VHA utilization; this analysis only included variables significantly associated with primary VHA health care use in bivariate analyses (P<.01). A post hoc regression analysis identified individual medical conditions that were associated with health care utilization. Finally, a relative importance analysis quantified the relative variance in VHA utilization explained by each of the statistically significant variables identified in the regression analysis.
RESULTS
Descriptive Statistics
Overall, among 4,069 participants, 20.5% (95% CI, 18.9–22.3%) reported that VHA was their main source of health care. The sample was 90.2% male and 78.1% white, 11.2% black, 6.6% Hispanic, and 4.2% other race, with a mean age of 62.2 years (SD = 15.7). Nearly, one-third (32.7%) reported completing a college degree or some higher education, 58.5% reported a household income over $60,000, and 72.4% reported being married or living with a partner.
Bivariate Group Comparisons
Table 1 shows sociodemographic and military characteristics by primary VHA utilization status. Compared to non-VHA users, primary VHA users were younger, more likely to be black/African American, less likely to be married/living with a partner, and less likely to have an annual household income over $60,000. They were also more likely to have enlisted in the service (versus being drafted or commissioned) and to have served in combat roles. Only 13.8% of primary VHA users reported having insurance through a current or former employer compared to nearly half (48.5%) of non-VA users.
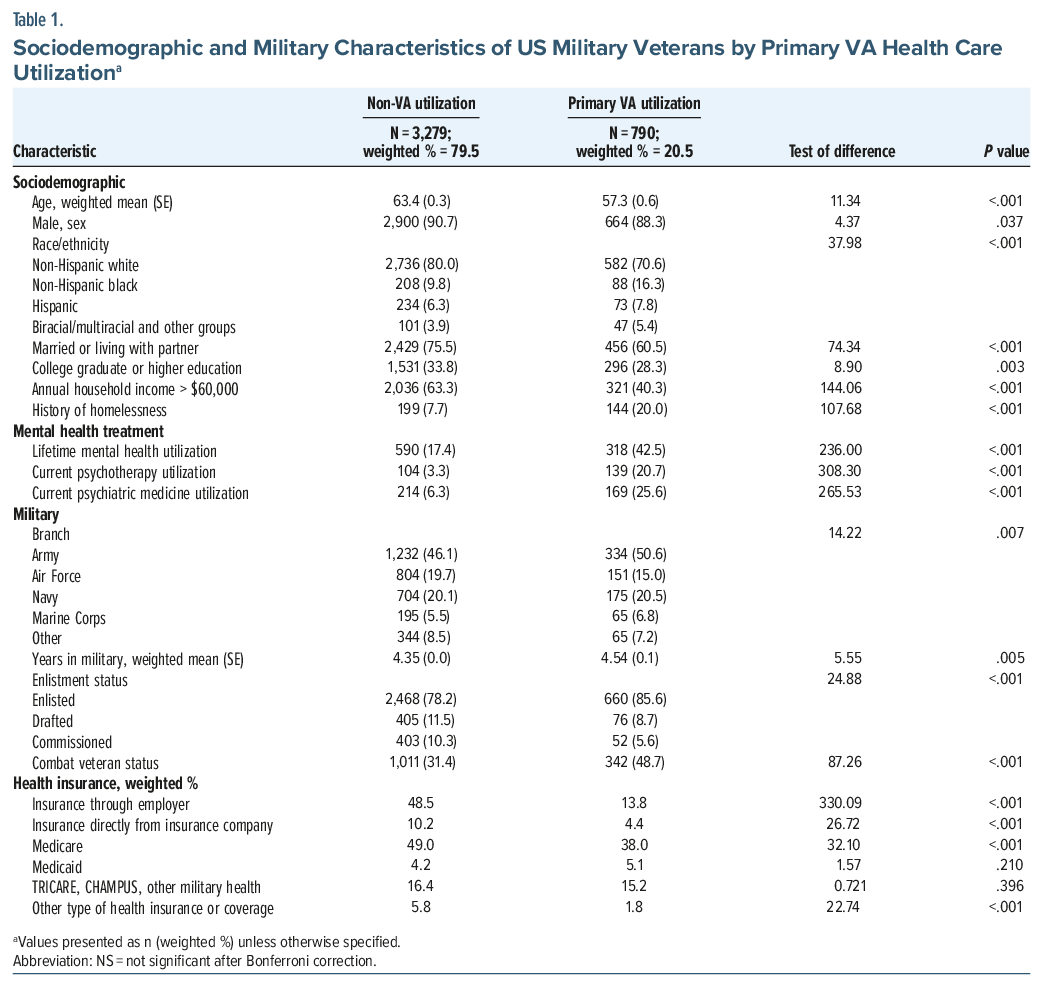
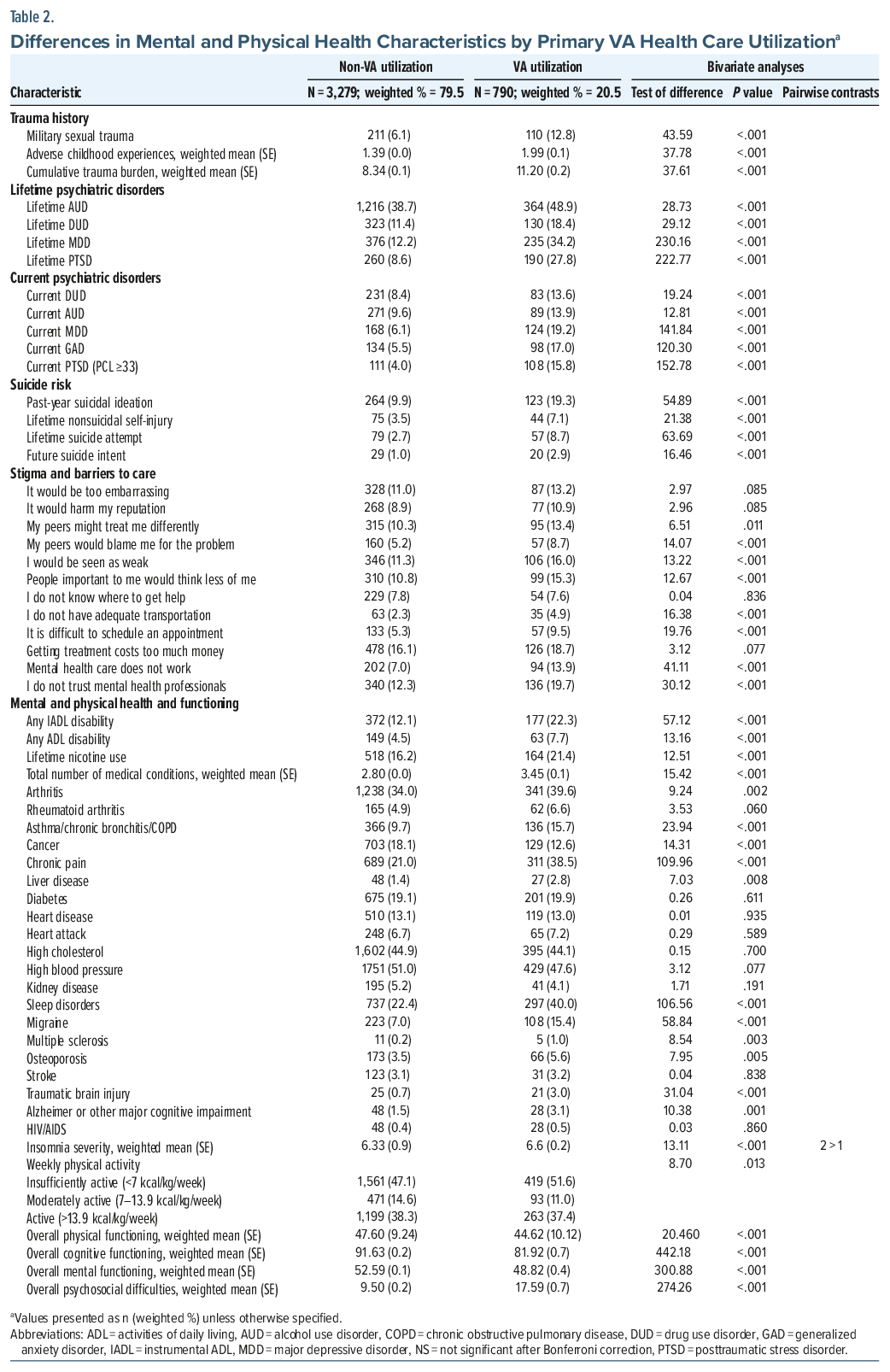
Primary VHA users reported higher rates of military sexual trauma, greater cumulative trauma, and more ACEs. They were more likely to screen positive for lifetime and current alcohol use disorder, drug use disorder, MDD, PTSD, and generalized anxiety disorder, and they had significantly higher suicide risk indicators (including past-year suicidal ideation, lifetime nonsuicidal self-injury, suicide attempts, and future suicidal intent). Primary VHA users were more likely than non-VHA users to report having a disability and a greater number of medical conditions, particularly sleep disorders, migraines, chronic pain, respiratory disorders, and TBI; they were, however, less likely to report a history of cancer. VHA users also scored lower on measures of mental, physical, and cognitive functioning and higher on a measure of psychosocial difficulties.
Primary VHA users also reported greater perceptions of stigma and barriers to mental health care. Specifically, they were more likely to endorse concerns that peers would treat them differently, see them as weak, or think less of them if they sought mental health care. They also more often endorsed logistical barriers to care (eg, transportation, scheduling), worries that mental health treatment does not work, and distrust of mental health professionals.
Multivariable Logistic Regression Model
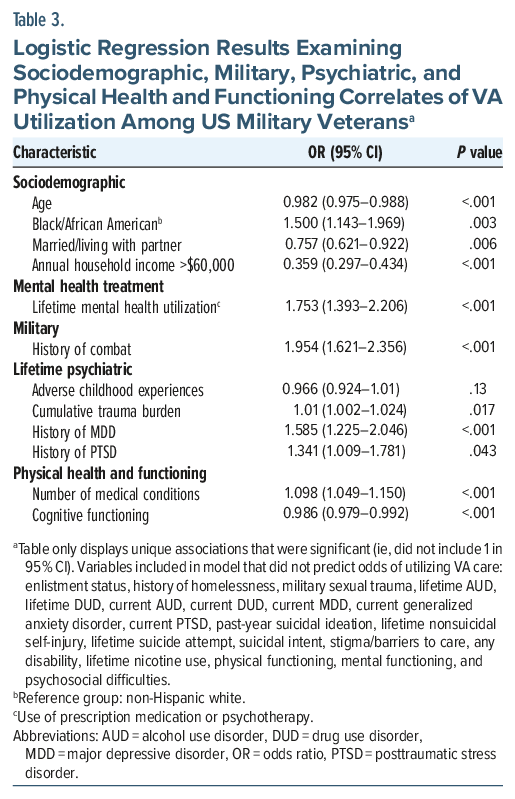
Results of a multivariable logistic regression analysis (Table 2) revealed several unique correlates of primary VHA health care utilization. Demographic and military-related predictors included younger age, black/African American race, being unmarried/unpartnered, having an annual household income ≤ $60,000, and combat exposure. Psychiatric correlates included greater cumulative trauma burden and a history of MDD or PTSD. Physical health correlates included a greater number of self-reported medical conditions and lower cognitive functioning. A planned post hoc analysis of individual provider-diagnosed medical conditions further indicated that chronic pain (odds ratio [OR]=1.45; 95% CI, 1.18–1.78), sleep disorders (OR =1.38; 95% CI, 1.13–1.70), and respiratory disorders (OR =1.31; 95% CI, 1.01–1.71) were independently associated with primary VHA health care use, while all other conditions were nonsignificant (Ps>.23) (Table 3).
Relative Importance Analysis
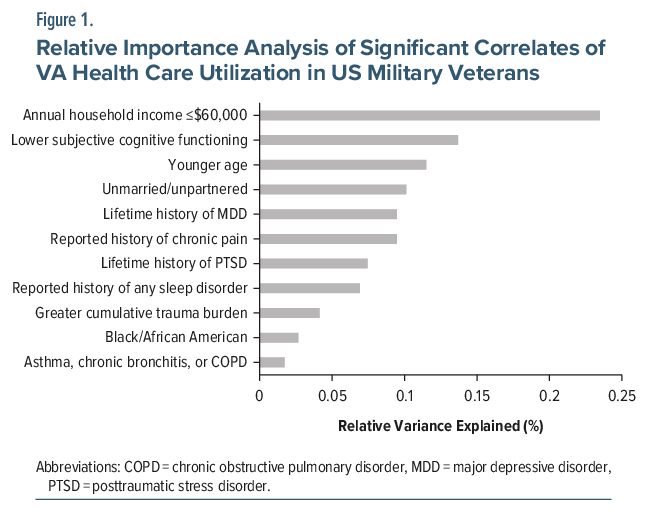
Finally, results of a relative importance analysis (Figure 1) revealed that the majority of the explained variance (Nagelkerke R2 = 0.23) in the model was accounted for by annual household income ≤$60,000 (23% relative variance explained [RVE]), lower self-reported cognitive functioning (14% RVE), younger age (11%), unmarried/unpartnered status (10%), lifetime history of MDD (9%), chronic pain (9%), lifetime history of PTSD (7%), and a sleep disorder diagnosis (6%).
DISCUSSION
This study sought to characterize the profile of an important subgroup of US military veterans who rely on the VHA as their primary source of health care in a nationally representative sample. Although prior work has described this population, contemporary data are needed given substantial demographic shifts in the veteran population and ongoing restructuring of the VA health care system. Overall, 1 of 5 veterans reported utilizing the VHA as their main source of health care, an increase from 16.9% in 2011.7 Consistent with earlier findings,16 primary VHA users were more likely to be younger, unmarried/unpartnered, and black/African American and to have lower household income (≤$60,000 annually). They also reported higher rates of depression and PTSD, greater trauma exposure, and a higher burden of chronic medical conditions such as chronic pain, sleep problems, and respiratory disorders. Collectively, these findings suggest that VHA users constitute a unique and vulnerable subgroup of veterans, characterized by more complex health needs and reduced financial and social resources, as well as greater barriers to mental health service engagement, including stigma, logistical challenges, and concerns about provider trust.
Several key differences emerged between primary VHA and non-VHA users. Lower household income was the strongest predictor, aligning with evidence that financial stressors such as housing insecurity, transportation barriers, and difficulty managing health care costs shape veterans’ reliance on the VHA.17 VHA programs, including travel reimbursement, housing initiatives, caregiver stipends, telehealth, and community-based outpatient clinics, represent important mechanisms for addressing these challenges.1 Expanding awareness of and access to such services remains particularly important for this subgroup.
Veterans who primarily used VHA services reported lower cognitive functioning, which can impair the ability to navigate complex health systems, understand treatment instructions, and adhere to medical regimens.18 This finding underscores the importance of cognitive screening, care coordination, and caregiver support. Veterans with lower cognitive functioning may rely on the VHA as a consistent and structured care provider, necessitating institutional adaptation to more frequent or longer appointments.6 The VHA offers “health care navigators” and other similar types of case management support for veterans using VA health care services.19
Younger and unmarried veterans were also more likely to rely on VHA services. Younger veterans often face distinct challenges, such as transitioning from military to civilian life, family reintegration, and pursuing education or career goals.20 They are also more likely to have served in post-9/11 conflicts, which are associated with higher rates of combat exposure, TBI, hearing loss, respiratory conditions, and mental health concerns.21 Further, unmarried/unpartnered veterans face additional risks of financial strain and housing insecurity,20 increased psychosocial stress, and lower social support.22 The VHA addresses these vulnerabilities through outreach programs, peer support services, and group-based interventions to foster connection and engagement.23
Mental health conditions, particularly MDD and PTSD, were strongly linked to primary VHA use. Both conditions are linked to significant functional impairment, heighted risk of suicidality, and poor occupational and interpersonal outcomes.24 In response, the VHA has expanded its mental health screening and intervention capacity and increased provider training in evidence-based treatments for mood and trauma-related disorders.5 Delivery of trauma-informed care is especially important given the elevated risk of retraumatization and treatment dropout in this population. For instance, studies have consistently documented lower retention rates for evidence-based trauma-focused therapies among veterans receiving VA care compared to civilian populations.25
Chronic medical conditions, including chronic pain, sleep, and respiratory disorders, were also elevated among VHA users. Veterans with chronic pain often experience reduced mobility, increased fatigue, and mood disturbances and may benefit from greater flexibility in treatment planning, as well as consideration of travel accessibility.26 The VHA is recognized as a leader in pain research and training, employing a stepped care model for pain management that accommodates a broad range of concerns across diverse care settings.27 Sleep problems further undermine functioning and treatment participation, necessitating targeted interventions such as cognitive-behavioral therapy for insomnia.28 Respiratory conditions, including asthma, chronic bronchitis, and chronic obstructive pulmonary disease, also remain a central focus of VHA care given veterans’ exposure to toxic substances during service (eg, burn pits, combustion products, sand, and dust particles). The VHA actively monitors respiratory health29 and provides specialized treatment. By addressing both medical and mental health concerns within one integrated health care system, the VHA is uniquely positioned to manage the complex comorbidities common among veterans.5
These findings should be interpreted in light of several limitations. First, the data were collected in 2019–2020. While this provides more recent information on VHA health care usage than prior surveys, it does not capture developments that occurred after the onset of the COVID-19 pandemic, such as the rapid expansion of telehealth services.14 Second, the study relied on self-report measures, which introduces the possibility of inaccurate recall or underreporting of prior diagnoses. Third, when assessing reasons for not seeking mental health services, participants were not asked to specify whether these barriers applied to VHA-based or non–VHA-based care. Finally, VHA utilization was measured with a single item asking whether the VHA was the participant’s main source of health care, which did not distinguish between those who used the VHA as a secondary source of care and those who did not use it at all.
Despite these limitations, results of this study highlight that veterans who rely on VHA services generally present with more complex psychiatric, medical, and social care needs than those who do not, underscoring the necessity of responsive and adaptive health care delivery models. These findings demonstrate that the VHA continues to serve as a “safety net” for veterans. Veterans with such needs may particularly benefit from providers who are familiar with military culture, trained in managing multimorbidity, and equipped to address service-connected conditions and combat-related exposures.21 Results of this study also underscore the importance of promoting awareness of and potentially expanding services that are responsive to these complexities, including treatment planning and coordination with external health care providers and social services. Efforts should also target well-documented barriers to care, such as stigma, logistical obstacles, and mistrust of health care providers.30 Continued quality improvement monitoring of VHA care in comparison with benchmarked private systems should likewise be prioritized. Moreover, these complexities should be carefully considered when evaluating treatment outcomes. Greater symptom severity, co-occurring conditions, and psychosocial stressors have consistently been linked to poorer treatment response and additional barriers to care.30 Without accounting for these factors, evaluators risk attributing differences in outcomes between VHA and non-VHA care to service quality alone rather than to the clinical and social contexts in which care is delivered.
Overall, veterans who primarily use VHA services represent a particularly vulnerable group that may require continued investment and attention to address their clinical and social needs. This subgroup is well-positioned to benefit from the tailored, accessible, integrative, and trauma-informed services that the VHA provides, as well as from opportunities for enhanced social and functional support. These insights should inform future VA outreach, resource allocation, and service delivery, with the ultimate goal of better meeting the complex and multifaceted needs of its core user population. Future research and policy should prioritize ongoing monitoring of VHA users to identify evolving needs, along with rigorous evaluation of new program development, integrated care models, and service innovations designed to improve access, quality, and outcomes in this population.
Article Information
Published Online: June 18, 2026. https://doi.org/10.4088/PCC.25m04176
© 2026 Physicians Postgraduate Press, Inc.
Submitted: December 24, 2025; accepted February 24, 2026.
To Cite: Meshberg-Cohen S, Goodwin SR, Fischer IC, et al. Primary users of the VA health care system: prevalence, correlates, and implications for care delivery. Prim Care Companion CNS Disord 2026;28(3):25m04176.
Author Affiliations: Psychology Service, VA Connecticut Healthcare System, West Haven, Connecticut (Meshberg-Cohen, Goodwin, Pietrzak, Fischer); Department of Psychiatry, Yale School of Medicine, New Haven, Connecticut (Meshberg-Cohen, Fischer, Cook, Tsai, Pietrzak); National Center for PTSD, VA Connecticut Healthcare System, West Haven, Connecticut (Meshberg-Cohen, Fischer, Pietrzak); Department of Management, Policy and Community Health, School of Public Health, University of Texas Health Science Center at Houston, Houston, Texas (Tsai); National Center on Homelessness Among Veterans, U.S. Department of Veterans Affairs, Washington, DC (Tsai); Department of Social and Behavioral Sciences, Yale School of Public Health, New Haven, Connecticut (Pietrzak).
Corresponding Author: Sarah Meshberg-Cohen, PhD, VA Connecticut Healthcare System, 950 Campbell Ave, Mailstop: 116B, West Haven, CT 06516 ([email protected]).
Financial Disclosure: None.
Funding/Support: None. The National Health and Resilience in Veterans Study is supported by the US Department of Veterans Affairs National Center for PTSD.
ORCID: Sarah Meshberg-Cohen: https://orcid.org/0000-0003-1719-3681; Shelby R. Goodwin: https://orcid.org/0000-0003-2863-0007; Ian C. Fischer: https://orcid.org/0000-0002-7343-071X; Joan M. Cook: https://orcid.org/0000-0001-7509-9760; Jack Tsai: https://orcid.org/0000-0002-0329-648X; Robert H. Pietrzak: https://orcid.org/0000-0002-5561-6414
Supplementary Material: Available at Psychiatrist.com.
Clinical Points
- One in 5 veterans reported using the Veterans Affairs (VA) as their primary source of health care.
- Veterans who use VA services represent a particularly vulnerable group who tend to experience more complex psychiatric and medical needs.
- Comprehensive, integrated services are needed for those who rely on VA health care.
References (30)

- Lunetta F, Stern J, McNamee L. Addressing Untimely Healthcare Access of Veterans Receiving Care Through the Veteran Healthcare Administration (VHA). School Professional Studies; 2024. 22. https://commons.clarku.edu/graduate_school_professional_studies/22
- Tsai J, Mehta K, Hunt-Johnson N, et al. Experiences and knowledge of US Department of Veterans Affairs clinical services, research, and education: results from a national survey of veterans. J Public Health Management Pract. 2021;27(2):173–185. CrossRef
- Apaydin EA, Paige NM, Begashaw MM, et al. Veterans health administration (VA) vs. non-VA healthcare quality: a systematic review. J Gen Intern Med. 2023;38(9):2179–2188.
- Eibner C, Krull H, Brown KM, et al. Current and projected characteristics and unique health care needs of the patient population served by the Department of Veterans Affairs. Rand Health Q. 2016;5(4):13. PubMed
- Etingen B, Smith BM, Zeliadt SB, et al. VHA whole health services and complementary and integrative health therapies: a gateway to evidence-based mental health treatment. J Gen Intern Med. 2023;38(14):3144–3151. CrossRef
- Yoon J, Phibbs CS, Ong MK, et al. Outcomes of veterans treated in veterans affairs hospitals vs non–veterans affairs hospitals. JAMA Netw Open. 2023;6(12):e2345898.
- Meffert BN, Morabito DM, Sawicki DA, et al. US veterans who do and do not utilize veterans affairs health care services: demographic, military, medical, and psychosocial characteristics. Prim Care companion CNS Disord. 2019;21(1):26992.
- Atkins D, Kilbourne AM, Shulkin D. Moving from discovery to system-wide change: the role of research in a learning health care system: experience from three decades of health systems research in the Veterans Health Administration. Annu Rev Public Health. 2017;38(1):467–487. PubMed CrossRef
- Mattocks KM, Cunningham K, Elwy AR, et al. Recommendations for the evaluation of cross-system care coordination from the VA state-of-the-art working group on VA/non-VA care. J Gen Intern Med. 2019;34(Suppl 1):18–23. PubMed CrossRef
- Bureau USC. American Community Survey, ACS 1-Year Estimates Subject Tables. Table S2101. https://data.census.gov/table/ACSST1Y2011.S2101?q=S2101. Accessed July 27, 2025
- 400. 000+ Veterans enrolled in VA health care over past 365 days, 30% increase over last year. 2024. https://news.va.gov/press-room/va-enrolled-401006-veterans-healthcare-365/. Accessed March 25, 2025
- Vanneman ME, Wagner TH, Shwartz M, et al. Veterans’ experiences with outpatient care: comparing the Veterans Affairs system with community-based care: study compares veterans’ experiences in VA-delivered and community-based outpatient care. Health Aff. 2020;39(8):1368–1376.
- Bokhour BG, Haun JN, Hyde J, et al. Transforming the veterans affairs to a whole health system of care: time for action and research. Med Care. 2020;58(4):295–300. PubMed CrossRef
- Pierce BS, Perrin PB, Tyler CM, et al. The COVID-19 telepsychology revolution: a national study of pandemic-based changes in US mental health care delivery. Am Psychol. 2021;76(1):14–25. CrossRef
- Pietrzak RH, Levy BR, Tsai J, et al. Successful aging in older US veterans: results from the 2019–2020 national health and Resilience in veterans study. Am J Geriatric Psychiatry. 2021;29(3):251–256. CrossRef
- Fink DS, Stohl M, Mannes ZL, et al. Comparing mental and physical health of US veterans by VA healthcare use: implications for generalizability of research in the VA electronic health records. BMC Health Serv Res. 2022;22(1):1500. CrossRef
- Elbogen EB, Zeber JE, Vogt D, et al. Financial status and well-being in recently separated military veterans. Mil Med. 2023;188(7-8):e2181–e2188.
- Maye JE, Depp CA, Lee EE, et al. Cognition and functional capacity: an initial comparison of veteran and non-veteran older adults. Mil Med. 2024;189(9-10):1864–1870. CrossRef
- Felderhoff B, Wagner B. The veteran community navigator program: Filling Gaps for veterans in transition. J Soc Serv Res. 2025:1–19.
- Montgomery AE, Tsai J, Blosnich JR. Demographic correlates of veterans’ adverse social determinants of health. Am J Prev Med. 2020;59(6):828–836.
- Na PJ, Schnurr PP, Pietrzak RH. Mental health of U.S. combat veterans by war era: results from the National Health and Resilience in Veterans Study. J Psychiatr Res. 2023;158:36–40. CrossRef
- Vaingankar JA, Abdin E, Chong SA, et al. The association of mental disorders with perceived social support, and the role of marital status: results from a national cross-sectional survey. Archives Public Health. 2020;78(1):108. PubMed CrossRef
- Drebing CE, Reilly E, Henze KT, et al. Using peer support groups to enhance community integration of veterans in transition. Psychol Serv. 2018;15(2):135–145.
- Nichter B, Norman S, Haller M, et al. Psychological burden of PTSD, depression, and their comorbidity in the US veteran population: suicidality, functioning, and service utilization. J Affect Disord. 2019;256:633–640. PubMed CrossRef
- Varker T, Jones KA, Arjmand H-A, et al. Dropout from guideline-recommended psychological treatments for posttraumatic stress disorder: a systematic review and meta-analysis. J Affect Disord Rep. 2021;4:100093. CrossRef
- Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097.
- Courtney RE, Schadegg MJ. Chronic, noncancer pain care in the veterans administration: current trends and future directions. Anesthesiol Clin. 2023;41(2):519–529.
- Folmer RL, Smith CJ, Boudreau EA, et al. Prevalence and management of sleep disorders in the veterans health administration. Sleep Med Rev. 2020;54:101358. PubMed CrossRef
- Dursa EK, Tadesse BE, Carter CE, et al. Respiratory illness among Gulf war and Gulf war era veterans who use the Department of veterans affairs for healthcare. Am J Industrial Med. 2020;63(11):980–987. PubMed CrossRef
- Ein N, Gervasio J, St. Cyr K, et al. A rapid review of the barriers and facilitators of mental health service access among Veterans and their families. Front Health Serv. 2024;4:1426202.
Please sign in or purchase this PDF for $40.




