Abstract
Objective: To determine the prevalence of generalized anxiety disorder (GAD) in patients (aged 18–86 years, not under treatment, and with no prior diagnosis of GAD) attending an underserved primary care outpatient clinic in Higuerote, Venezuela, between October and December 2023.
Methods: A descriptive, cross-sectional, quantitative, population-based study was conducted. Data were collected via a 49-item closed-question survey that included the Hamilton Anxiety Rating Scale, Perceived Stress Scale, and 16 author-designed yes/no questions on GAD-related risk factors. Statistical analysis was performed using SPSS V26; P < .01 was considered statistically significant.
Results: The study included 440 patients (mean age of 33.8± 15.3 years; 70.2% female); 50.0% of participants presented with mild anxiety, 6.0% with mild-to-moderate anxiety, and 44.0% with moderate-to-severe anxiety. Psychosocial stress, reported by 299 patients (67.9%), was strongly associated with anxiety severity (odds ratio [OR] =124.6; 99% CI, 29.3–529.6; P<.001). Among those with moderate-to-severe anxiety, 85.7% (n=192; OR= 641.0; 99% CI, 138.5–2,966.8; P<.001) reported anxiety episodes, and 90.0% (n= 180; OR= 74.9; 99% CI, 30.2–185.7; P<.001) reported panic attacks. Alcohol consumption (71.8%, n=316) was significantly associated with anxiety severity (P<.001). Family history of anxiety (60.0%, n=264) and depression (51.8%, n=228) were also significantly associated with anxiety severity (P<.01). While SARS-CoV-2 was infection was significantly associated with anxiety severity (OR=1.9; 99% CI, 1.2–3.1; P<.001), history of traumatic brain injury was not (P = .12).
Conclusions: This study revealed a statistically significant high prevalence of GAD in the underserved population of Higuerote, Venezuela. These results show the need for updated mental health epidemiologic data, surveillance, and individualized community-based strategies in disadvantaged/marginalized populations, by empowering local psychiatric workforces through data-driven, context-specific care initiatives.
Prim Care Companion CNS Disord 2026;28(3):25m04168
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
The lack of updated official epidemiologic data on mental health disorders is a critical reality that is currently affecting Venezuela. It is no secret that the mental health of Venezuelans has been negatively impacted due to its sociopolitical, cultural, economic, and humanitarian crisis.1,2 Mental health disorders have been increasing markedly in this new post–COVID-19 era, particularly anxiety, depression, and posttraumatic stress disorder (PTSD).3 It is estimated that around 300 million people worldwide suffer from generalized anxiety disorder (GAD), which is defined as an excessively disruptive, intrusive, egodystonic, out-of-control worry about multiple ordinary, day-to-day situations and domains during at least a 6-month period that may cause physical symptoms, including restlessness, fatigue, muscle tension, irritability, sleep disturbances, difficulty concentrating, gastrointestinal symptoms, and chronic headaches. GAD currently has a worldwide incidence of 10%–20% and a prevalence increase of 28% due to the COVID-19 pandemic.3–6
According to the 2023 annual unofficial PsicoData study, carried out by the Andrés Bello Catholic University in Caracas, Venezuela, 90% of Venezuelans suffer from GAD, of whom 64% state that the main source of their worry is economic problems; however, the PsicoData report used a symptom-based screening questionnaire, rather than the then current Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, diagnostic criteria for GAD. Likewise, in 2022, the Venezuelan Violence Observatory reported a total of 2,173 suicides, estimating an underreporting of 49.2% according to the official reviews of the mortality yearbooks; Miranda State ranked fourth among the states with the highest suicide rates in Venezuela.7,8 This is no coincidence, considering that 86% of people with GAD live in third world nations with little to no access to primary care, such as Venezuela, and have not received specific pharmacotherapy for their mental health disorders.4
Due to the limited information available on GAD in Venezuela, it was imperative to study and understand the consequences that this psychiatric disorder might have on Venezuelans. We conducted a study on the prevalence of GAD in patients that attended the Pronto Socorro primary care outpatient clinic, the only institution to offer outpatient consultations to the underserved population of Higuerote, Miranda State, Venezuela, describing how this community is exposed to a constant daily state of anxiety and stress, exacerbated by traumatic brain injuries, post–COVID-19 syndrome, and the socioeconomic/humanitarian crisis affecting the country and Miranda State.
METHODS
Study Design
A descriptive, cross-sectional, quantitative, and population-based study was conducted to determine the prevalence of GAD in patients who attended the Pronto Socorro primary care outpatient clinic between October and December 2023.
Survey Design and Data Collection
Data were obtained using an anonymous 49-item closed-question survey created by the authors in the Google Forms platform. The survey was preceded with an introduction, establishing that all the bioethical principles of autonomy, beneficence, nonmaleficence, and justice were taken into account, respecting the confidentiality and anonymity of the studied and surveyed sample, with no coercion or violence, with equity, and with no privileges given to one over the other.
The survey was structured into 4 parts. Part 1 included the respondent’s affiliation data (age, sex, and profession), always respecting the patient’s confidentiality. Part 2 presented a total of 14 closed questions, extracted directly from the Hamilton Anxiety Rating Scale (HAM-A),9 evaluating anxious mood, tension, fear, sleep disorders, intellectual disorders, depression, muscular symptoms, sensory symptoms, cardiovascular symptoms, gastrointestinal symptoms, respiratory symptoms, genitourinary symptoms, vegetative symptoms, and behavior at the time of the survey. Each symptom was quantified on a 0-to-4–point scale, with 0: absent, 1: mild, 2: moderate, 3: severe, and 4: very severe. The sum varied between 0 and 56 points, where a score <17 indicated mild symptoms; between 18 and 24, mild-to-moderate symptoms; and >25, moderate-to-severe symptoms. For Part 3, the authors used the Perceived Stress Scale (PSS)10—a specific 10-question screening tool that measures and quantifies psychosocial stress within a range of 0 and 40 points; ≤13 points indicates absent or low levels of stress, while ≥14 points represents moderate to severe levels of stress. Part 4 consisted of 16 “yes” or “no” questions developed by the authors and related to possible GAD risk factors and comorbidities, including family history of anxiety, traumatic childhood events, personal and family history of depression, smoking habits and alcohol and illicit substance consumption, comorbidities, eating habits, history of SARS-CoV-2 infection, history of head trauma, and history of anxiety and panic attacks.
The study was approved by the Ethics Committee of the Faculty of Medicine of Universidad Central de Venezuela. The survey was sent electronically to those who agreed to participate. Participation was voluntary and anonymous.
Sample
Inclusion criteria included (1) age ≥18 years, (2) not currently receiving psychiatric pharmacotherapy, and (3) no prior diagnosis of GAD. Exclusion criteria included inability to provide informed consent, incomplete survey responses, or failure to meet any of the inclusion criteria. Participation was offered consecutively to all patients meeting inclusion criteria during the study period. Of 459 patients who were invited, 440 completed the survey and met inclusion criteria, yielding a response rate of 95.6%. The survey was administered via Google Forms and was accessible via cell phone or tablet. Patients were allowed to complete the survey only once; no repeated entries were included.
Statistical Analysis
The data obtained were collected, downloaded, organized, and totaled using Microsoft Excel Version 2019 and subsequently analyzed using SPSS Version 26. Continuous variables were summarized as means and SDs, while categorical variables were expressed as frequencies and percentages. Associations between categorical variables were assessed using 2 × 2 contingency tables, with the calculation of odds ratios (ORs) and 99% CIs. Pearson χ2 test was used to determine statistical significance. Binary logistic regression analysis was performed to evaluate associations between anxiety levels and relevant risk factors. Statistical significance was set at P<.01. Given the cross-sectional design, ORs were interpreted as measures of association rather than risk. Variables with conceptual overlap with anxiety severity were interpreted cautiously.
RESULTS
A total of 440 participants met the inclusion criteria and were included in the final analysis. The mean age of the patients was 33.75±15.307 (range, 18–86 years), and the majority were female (70.21%, n=308).
Anxiety Severity
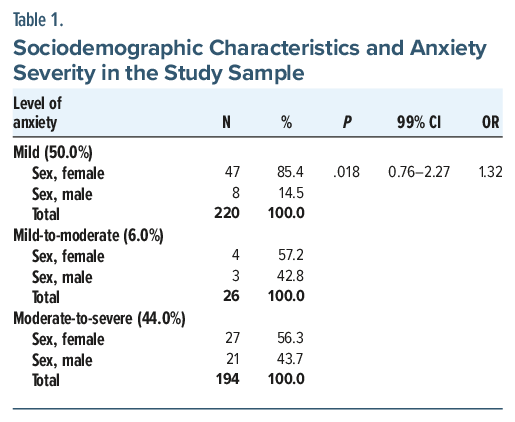
Based on HAM-A scores, 50.0% of the sample (n =220) was classified as having mild anxiety, 44.0% (n =194) moderate-to-severe anxiety, and 6.0% (n=26) mild-to-moderate anxiety. Female sex predominated across all anxiety categories (85.4%, n=47; 56.3%, n=27; and 57.2%, n=4, respectively). No statistically significant association was observed between sex and anxiety severity after adjustment (OR=1.32; 99% CI, 0.76–2.27; P =.018), as seen in Table 1.
Psychosocial Stress
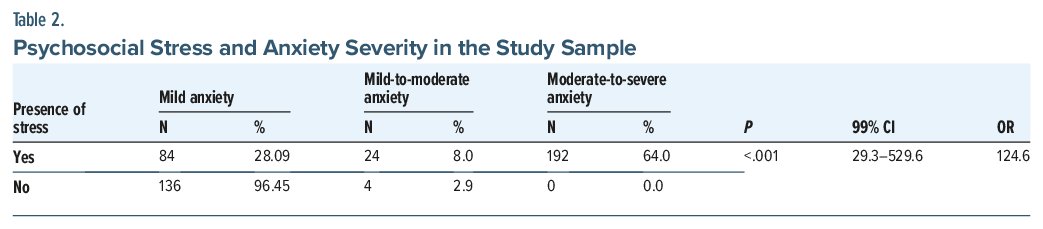
Psychosocial stress, as measured by the PSS, was reported by more than half of the total sample (67.9%; n=299), among which 53.17% (n= 40) reported moderate stress levels, 44% (n =132) mild stress levels, and 2.6% (n=8) severe stress levels. On the other hand, as noted in Table 2, 64.0% of those patients that suffered from stress (n =192) also had moderate-to-severe anxiety; 28.09% (n=84) had mild anxiety, and 8.0% (n =24) had mild-to-moderate anxiety. Psychosocial stress was strongly associated with anxiety severity (OR =124.6; 99% CI, 29.3–529.6; P<.001).
Anxiety Episodes and Panic Attacks
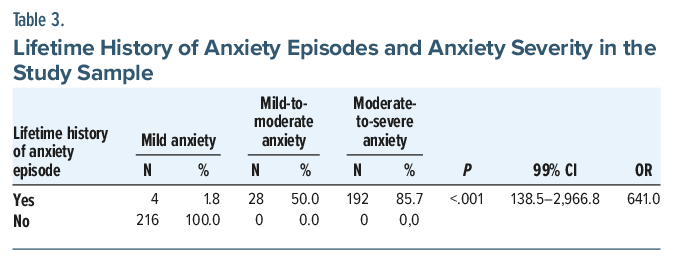
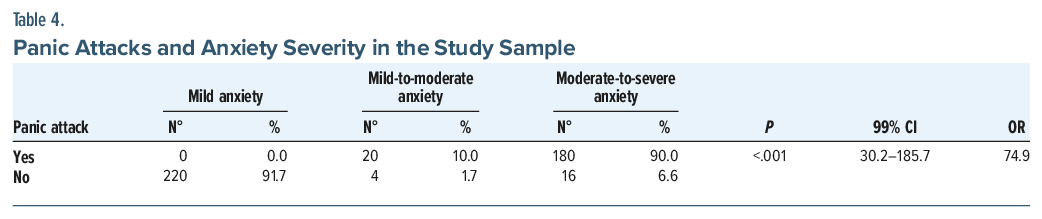
It is important to take into account that 50.9% (n =224) of the sample reported a lifetime history of anxiety episodes, while 49.1% (n=216) reported at least 1 lifetime panic attack. Among patients with moderate-to-severe anxiety, 85.7% (n=192) reported anxiety episodes, and 90.0% (n=180) reported panic attacks, showing a statistical association among the variables (OR =641.0; 99% CI, 138.5–2,966.8; P<.001 and OR=74.9; 99% CI, 30.2–185.7; P <.001, respectively), as shown in Table 3 and Table 4. Large ORs with wide CIs were observed for anxiety episodes and panic attacks, reflecting strong co-occurrence rather than independent risk.
Substance Use
Alcohol consumption was reported by 77.8% of participants (n=316), 58.22% (n=184) of whom consumed occasionally, especially on weekends, while the remaining 41.77% (n=132) drank alcoholic beverages at least once a month or less. In that sense, 78.30% (n=148), 63.63% (n=140), and 100% (n=28) of patients with moderate-to-severe anxiety, mild anxiety, and mild-to-moderate anxiety, independently, consume alcohol. Alcohol use was significantly associated with anxiety severity (OR=3.4; 99% CI, 1.8–6.2; P<.001). Smoking habits were reported by 14.5% of participants (n=64) and illicit substance use by 2.0% (n=9); these variables did not show a statistically significant association with anxiety severity.
Family History and Comorbidities
A family history of anxiety was reported by 60.0% of participants (n=264), and a family history of depression was reported by 51.8% (n=228). Both were significantly associated with anxiety severity (OR=2.9; 99% CI, 1.6–5.2; P < .01, and OR=2.1; 99% CI, 1.2–3.8; P < .01, respectively). A personal history of depression and traumatic childhood event were reported by 13.2% (n=58) and 47.9% (n=211) of the sample, respectively, and were not significantly associated with anxiety severity.
Of all the surveyed patients, only 22.7% of participants (n=100) reported at least 1 medical comorbidity, most commonly arterial hypertension (44.0%, n=44) and asthma (40.0%, n=40), followed by diabetes mellitus (16.0%, n=16). The presence of medical comorbidities was not significantly associated with anxiety severity.
Eating Habits
More than half of the sample (53.6%, n=236) reported unbalanced eating habits, including skipping 1 or more daily meals. Additionally, 85.7% (n =376) reported consumption of sweets, fast food, or ultraprocessed foods in moderate (64.89%, n=244), small (31.91%, n=120), or large (3.19%, n=12) amounts 1 to 3 times (72.34%, n=272), once or less (24.46%, n=92), or more than 3 times (3.9%, n=12) per week, respectively. Unbalanced eating habits were significantly more frequent among patients with moderate-to-severe anxiety and were associated with higher anxiety severity (P< .01).
SARS-CoV-2 Infection
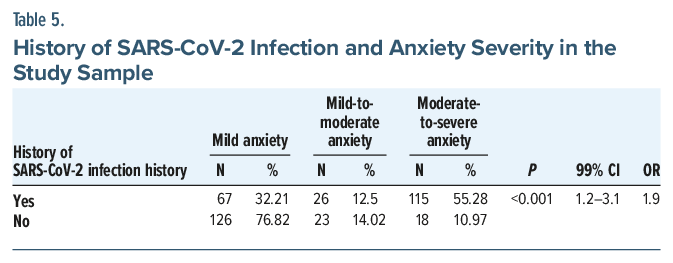
A history of SARS-CoV-2 infection was reported by 47.27% of participants (n=208), of whom 84.2% (n=175) reported that the infection occurred more than 1 year before the survey was carried out, with just 21.15% (n =44) requiring hospitalization. Symptoms were reported by 66.8% (n =139) of those that had the infection; the most frequent symptoms were fever, myalgia, allodynia, diarrhea, headaches, dyspnea, dysphagia, and nausea and vomiting (41.0%; n=57); fever, myalgia, allodynia, diarrhea, and headaches only (23.0%; n=32); and fever, dyspnea and severe headaches only (36.0%; n= 50). Among these individuals, 55.3% (n=115) had moderate-to-severe anxiety, 32.2% (n=67) had mild anxiety, and 12.5% (n=26) had mild-to-moderate anxiety. A history of SARS-CoV-2 infection was significantly associated with anxiety severity (OR=1.9; 99% CI, 1.2–3.1; P < .001), as shown in Table 5.
Traumatic Brain Injury
Only 10% of the sample (n =44) reported a history of traumatic brain injury, most of which occurred more than 10 years prior to the survey. Within this subgroup, 84.1% (n=37) had mild anxiety, and 15.9% (n=7) had mild-to-moderate anxiety; no cases of moderate-to-severe anxiety were observed. Due to the small and likely unrepresentative sample, bivariate and logistic analyses were not performed. Most reported injuries were remote, and recall bias may influence these results.
DISCUSSION
This study is the first, to the best of our knowledge, to assess the prevalence of GAD in Higuerote, one of Venezuela’s most underserved communities, and to analyze the correlation between GAD, SARS-CoV-2 infection, and traumatic brain injury in Venezuela. The most recent study conducted on the prevalence of GAD in Venezuela was carried out in 2017 by the Complutense University of Madrid11 in a sample of 814 patients who attended a primary care center in Caracas, the capital of Venezuela. The results were not statistically significant, with a prevalence of GAD and major depressive disorder of 10.6% and 7.0%, respectively; unlike our sample, in which mild (85.4%), moderate (57.2%), and severe (56.3%) GAD prevailed in women.
In a cross-sectional study by Chen et al12 assessing health care workers during the COVID-19 outbreak in China, moderate-to-severe anxiety was observed in 16.6% of participants using the GAD 7-item scale, compared to 44.0% in our study using the HAM-A. Similarly, mild anxiety was reported in 30.38% of participants in the Chinese study,12 compared to 50.0% in our sample. Likewise, the reported prevalence of moderate (14.2%) and mild (18%) stress by Ozamiz-Etxebarria et al13 during the outbreak of COVID-19 in Spain, measured via the Depression Anxiety Stress Scale, was not statistically significant, compared to our study in which the prevalence of psychosocial stress, measured by the PSS, was 65.0%, mild stress was 44.0%, moderate stress was 53.17%, and severe stress was 2.6%.
Unlike family history of depression (51.8%), a personal history of depression in our sample (13.2%) was not significantly associated with anxiety severity, which was similar to the prevalence of depression reported by Marsiglia et al14 in their sample of 1,159 Venezuelans from Caracas (7.6%). However, with a prevalence of 71.8% in our study, alcohol consumption was statistically significant, not only compared to smoking habits (14.54%) and illicit substance use (2.04%) in our sample, but also to a study conducted in Australia by Andrews et al,15 who, citing previously published data, reported an annual prevalence of 4.7% for alcohol dependence and 2.2% for drug dependence based on ICD-10 criteria in the UK population. Our results showed that GAD in the population of Higuerote is closely related to alcohol consumption, with a prevalence of 63.63%, 100%, and 78.3% in patients with mild, moderate, and severe anxiety, respectively.
The comorbidities that prevailed in 22.72% of our sample were high blood pressure (44.0%) and asthma (40.0%), similar to findings reported by Cruz16 (high blood pressure: 40.0%) and Chérrez et al17 (asthma: 36.0%). Both of these pathologies tend to appear and exacerbate in psychiatric disorders, especially in the presence of anxiety and stress, acting as risk factors of said conditions due to autonomic dysfunction and the intricate bidirectional interactions between the nervous system and the respiratory and immune systems.18–20
A correlation between the prevalence of anxiety and eating habits was found in our sample, with the consumption of carbohydrates and fats (85.7%), proinflammatory foods rich in C-reactive protein and interleukin-6, which is common in patients with mental health disorders due to an increase of oxidative stress, excessive production of free radicals, insulin resistance, and inflammatory processes, causing weight gain and thus exacerbating anxiety symptoms. Obese patients are 80% more likely to suffer from anxiety, and anxious patients are 58% more likely to suffer from obesity.21,22
It is important to take into account that 50.9% and 49.09% of our sample reported having suffered from at least 1 episode of anxiety and panic attacks, respectively, during their lifetime, which was much higher than that reported by Ozamiz-Etxebarria et al13 (22.5% and 24.0%, respectively), demonstrating a worrying increase in the prevalence of GAD both in Venezuela and worldwide, especially after the COVID-19 pandemic. Several factors may explain the increase in Higuerote, including the socioeconomic and humanitarian crisis that has affected Venezuela, particularly its underserved communities, in the past years; decreased quality of life in this population due to the destruction of public and private services; shortage of basic products and medicines; lack of opportunities in the region due to the massive exodus to Caracas; hyperinflation; lack of citizen’s safety; and posttraumatic stress generated by the COVID-19 pandemic, all of which tend to have an impact on the mental health of the population and resulting in GAD in these individuals.2
The COVID-19 pandemic must be highlighted, since it represented another challenge for the world population, and an even greater challenge for Venezuela, resulting in a state of physical and emotional overload that predisposed its inhabitants to suffer from GAD, depression, and PTSD, significantly diminishing their quality of life.23 Similar to studies by Alacevich et al,24 Schou et al,25 Hawes et al,26 and Lee et al,27 a correlation between GAD and SARS-CoV-2 infection—as a neuropsychiatric and proinflammatory disease28—was evidenced in our study, where almost half of the sample (47.27%) had a history of said infection, with 66.8% of them being symptomatic, and 33.21%, 12.5%, and 55.28% reporting mild, moderate, and severe anxiety, respectively.
Finally, the correlation between GAD and a history of traumatic brain injury in our study was not statistically significant, possibly due to a prevalence of only 10.0%, differing enormously with the data published by Alway et al29 (62.0%) in Australia, as well as with the results reported in meta-analyses published by Morse and Garner,30 Ahmed et al,31 Howlett et al,32 and Zgaljardic et al.33 Few studies have reported the psychiatric consequences of a traumatic brain injury; it is believed that these accidents may cause and exacerbate persistent cognitive deficiencies, causing mental health disorders. A more thorough and specific study should be carried out to understand the psychiatric implications of traumatic brain injuries.34
Limitations
The magnitude of the OR, particularly for anxiety episodes and panic attacks, should be interpreted with caution due to the cross-sectional nature of the study, potential sparse cell effects, and conceptual overlap between anxiety severity and these clinical features.
CONCLUSION
This study showed a statistically significantly high prevalence of GAD in the underserved population of Higuerote, Venezuela, especially in female patients, with mild anxiety, followed by moderate-to-severe and mild-to-moderate. There was a statistically significant correlation between GAD—particularly moderate-to-severe anxiety—and moderate stress, family history of anxiety and depression, occasional alcohol consumption, and unbalanced eating habits, unlike with depression, childhood history of traumatic events, smoking habits and illicit substance abuse, and presence of comorbidities among the respondents. The prevalence of anxiety and panic attacks and history of SARS-CoV-2 infection were also statistically significant in these patients, unlike history of traumatic brain injury, possibly due to the low number of patients that reported having suffered from such accidents. These results show the need for updated mental health epidemiologic data, surveillance, and individualized community-based strategies in disadvantaged/marginalized populations, by empowering local psychiatric workforces through data-driven, context-specific care initiatives. This study is limited by its cross-sectional design and the use of ORs, which may overestimate effect sizes in the presence of highly prevalent outcomes and sparse cells.
Article Information
Published Online: June 9, 2026. https://doi.org/10.4088/PCC.25m04168
© 2026 Physicians Postgraduate Press, Inc.
Submitted: December 17, 2025; accepted February 24, 2026.
To Cite: Carvallo Ruiz DE, Martínez Núñez EN, Cristancho Orlandino MC, et al. Empowering community psychiatry: a cross-sectional study of the prevalence of generalized anxiety disorder in an underserved Venezuelan population. Prim Care Companion CNS Disord 2026;28(3):25m04168.
Article Affiliations: Department of Psychiatry, BronxCare Health System, Icahn School of Medicine at Mount Sinai, Bronx, New York (Carvallo Ruiz, Gunturu); Faculty of Medicine, Universidad Central de Venezuela, Caracas, Venezuela (Martínez Núñez, Cristancho Orlandino).
Corresponding Author: Daniel Ernesto Carvallo Ruiz, MD, Department of Psychiatry, BronxCare Health System, Icahn School of Medicine at Mount Sinai, Bronx, New York ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
ORCID: Daniel Ernesto Carvallo Ruiz: https://orcid.org/0000-0002-5176-4436;
Elizabeth Natalia Martínez Núñez: https://orcid.org/0000-0003-4668-4586; Mariana
Carolina Cristancho Orlandino: https://orcid.org/0000-0002-8626-4618; Sasidhar
Gunturu: https://orcid.org/0000-0002-6867-2394
Clinical Points
- Generalized anxiety disorder is highly prevalent in underserved Venezuelan populations, particularly among women, highlighting the need for routine screening in primary care settings.
- Psychosocial stress, family history of anxiety or depression, occasional alcohol consumption, and unbalanced eating habits are key factors associated with moderate-to-severe anxiety; addressing these factors may improve patient outcomes through individualized interventions.
- Awareness of post–COVID-19 anxiety symptoms and early identification of anxiety and panic episodes can guide community-based and preventive mental health strategies, especially in resource-limited settings.
References (34)

- González MG. The health system crisis in Venezuela. Salus. 2018;22(1):6–7. https://www.redalyc.org/journal/3759/375956270002/html/. Accessed November 17, 2025
- Monitoring health Access in Venezuela: June 2019 Bulletin; 2019. Convite por la salud, Venezuela: Convite, A.C. Web Site https://issuu.com/conviteac/docs/bolet_n_23_convite. Accessed October 15, 2025.
- Mental health disorders. World Health Organization, Geneva: WHO Web Site. 2025. https://www.who.int/news-room/fact-sheets/detail/mental-disorders. Accessed October 15, 2025.
- Policy brief. COVID-19 and the need for action on mental health. In: UN Web Site. United Nations, New York; 2020. https://www.un.org/sites/un2.un.org/files/un_policy_brief-covid_and_mental_health_final.pdf. Accessed November 19, 2025
- Mental health and COVID-19. Pan American Health Organization. PAHO Web Site. Washington D.C.. https://www.paho.org/es/salud-mental-covid-19. Accessed September 30, 2025
- United Nations Sustainable Development Group [Internet]. The pandemic complicates the humanitarian crisis in Venezuela and neighboring countries. 2020. Available on:. https://unsdg.un.org/es/latest/stories/la-pandemia-complica-la-crisis-humanitaria-en-venezuela-y-los-paises-vecinos
- The impact of the economic crisis increases suicide rates in Venezuela. Venezuelan Violence Obs Web Site. https://observatoriodeviolencia.org.ve/news/la-huella-de-la-crisis-economica-eleva-los-suicidios-en-venezuela/. Accessed November 11, 2025
- A psychosocial portrait: Andrés Bello Catholic University. Department of Psychology. PsicoData Venezuela Web Site. https://psicologia.ucab.edu.ve/wp-content/uploads/2023/02/compressed.pdf. Accessed December 3, 2025
- Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. PubMed CrossRef
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396.
- Borges G, Taisa. Study on depression and anxiety using the PHQ in Venezuela. Docta Complutense; 2017. https://dialnet.unirioja.es/servlet/tesis?codigo=122945
- Chen J, Liu X, Wang D, et al. Risk factors for depression and anxiety in healthcare workers deployed during the COVID-19 outbreak in China. Soc Psychiatry Psychiatr Epidemiol. 2021;56(1):47–55. CrossRef
- Ozamiz-Etxebarria N, Dosil-Santamaria M, Picaza-Gorrochategui M, et al. Levels of stress, anxiety and depression in the first phase of the COVID-19 outbreak in a sample collected in northern Spain. Cad Saúde Pública. 2020;36(4):e00054020. PubMed CrossRef
- Marsiglia G. Italo. Clinical and epidemiological study of anxiety and depression in a sample of 1159 patients. Gac Méd Caracas. 2010;118(1).
- Andrews G, Henderson S, Hall W. Prevalence, comorbidity, disability and service utilisation. Overview of the Australian National Mental Health Survey. Br J Psychiatry. 2001;178:145–153. PubMed CrossRef
- Cruz A. Anxiety and depression in patients with high blood pressure. In: Santa Rosa Hospital. 2019. César Vallejo University: Faculty of Health Sciences-Professional School of Medicine; 2019. https://repositorio.ucv.edu.pe/bitstream/handle/20.500.12692/88277/Cruz_AAE-SD.pdf?sequence=1&isAllowed=y. Accessed November 30, 2025
- Chérrez I, Vanegas E, Félix M, et al. Influence of anxiety and depression on asthma control in Ecuadorian patients. Pilot Study Rev Alerg Méx:66(3). https://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S2448-91902019000300292. Accessed November 27, 2025
- Di Marco F, Santus P, Centanni S. Anxiety and depression in asthma. Curr Opin Pulm Med. 2011;17(1):39–44.
- Johnson HM. Anxiety and hypertension: is there a link? a literature review of the comorbidity relationship between anxiety and hypertension. Curr Hypertens Rep. 2019;21(9):66. CrossRef
- Liu MY, Li N, Li WA, et al. Association between psychosocial stress and hypertension: a systematic review and meta-analysis. Neurol Res. 2017;39(6):573–580. PubMed CrossRef
- Marx W, Lane M, Hockey M, et al. Diet and depression: exploring the biological mechanisms of action. Mol Psychiatry. 2021;26(1):134–150. CrossRef
- Gay V, Jiménez D, García J, et al. Association between anxiety, overweight and obesity in an adult population assigned to a family medicine unit. Aten Fam. 2020;27(3):131–134.
- Franco L, García M, Pinto L, et al. Mental health and COVID-19: prevalence of depression and anxiety in young adults in Latin America during the COVID-19 pandemic. Universidad del Norte, Barranquilla, Colombia. 2022. https://manglar.uninorte.edu.co/bitstream/handle/10584/10775/1140904570.pdf?sequence=1&isAllowed=y. Accessed November 30, 2025.
- Alacevich C, Thalmann I, Nicodemo C, et al. Depression and anxiety during and after episodes of COVID-19 in the community. Sci Rep. 2023;13(1):8257. CrossRef
- Schou TM, Joca S, Wegener G, et al. Psychiatric and neuropsychiatric sequelae of COVID-19 - A systematic review. Brain Behav Immun. 2021;97:328–348. CrossRef
- Hawes MT, Szenczy AK, Klein DN, et al. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol Med. 2022;52(14):3222–3230. CrossRef
- Lee H, Choi D, Lee JJ. Depression, anxiety, and stress in Korean general population during the COVID-19 pandemic. Epidemiol Health. 2022;44:e2022018. CrossRef
- Miller AH, Raison CL. The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nat Rev Immunol. 2016;16(1):22–34. PubMed CrossRef
- Alway Y, Gould KR, Johnston L, et al. A prospective examination of Axis I psychiatric disorders in the first 5 years following moderate to severe traumatic brain injury. Psychol Med. 2016;46(6):1331–1341. PubMed CrossRef
- Morse AM, Garner DR. Traumatic brain injury, sleep disorders, and psychiatric disorders: an underrecognized relationship. Med Sci (Basel). 2018;6(1):15. CrossRef
- Ahmed S, Venigalla H, Mekala HM, et al. Traumatic brain injury and neuropsychiatric complications. Indian J Psychol Med. 2017;39(2):114–121. CrossRef
- Howlett JR, Nelson LD, Stein MB. Mental health consequences of traumatic brain injury. Biol Psychiatry. 2022;91(5):413–420. CrossRef
- Zgaljardic DJ, Seale GS, Schaefer LA, et al. Psychiatric disease and post-acute traumatic brain injury. J Neurotrauma. 2015;32(23):1911–1925. CrossRef
- Mallya S, Sutherland J, Pongracic S, et al. The manifestation of anxiety disorders after traumatic brain injury: a review. J Neurotrauma. 2015;32(7):411–421. PubMed CrossRef
Please sign in or purchase this PDF for $40.