Abstract
Objective: To compare the efficacy of lorazepam and diazepam in managing alcohol withdrawal and associated anxiety and depressive symptoms in alcohol dependence syndrome.
Methods: Sixty male patients diagnosed with alcohol dependence syndrome (International Classification of Diseases, Eleventh Revision) were randomly assigned to receive lorazepam or diazepam using a symptom-triggered oral detoxification protocol. Baseline assessments included the Severity of Alcohol Dependence Questionnaire (mean score = 22.6 ± 4.81) and the Clinical Institute Withdrawal Assessment for Alcohol–Revised (mean CIWA-Ar score= 10.98±2.45). Anxiety and depression were measured using the Hamilton Anxiety Rating Scale (HAM-A) and Hamilton Depression Rating Scale (HAM-D) at baseline, postdetoxification, and 12 weeks. Benzodiazepines were gradually tapered and stopped after detoxification.
Results: Participants (mean age of 40.85 ± 8.30 years) showed comparable baseline withdrawal severity (CIWA-Ar P = .795) and similar reductions after detoxification (P = .999) and at 12 weeks (P = .321). Time to >50% symptom reduction was slightly shorter with diazepam (4.6 vs. 4.97 days; P = .241). Both groups demonstrated improvement in anxiety and depression, with slightly greater reductions in the lorazepam group, though differences were not statistically significant (HAM-A: P = .146; HAMD-D: P = .103).
Conclusions: Lorazepam and diazepam are equally effective in managing alcohol withdrawal.
Trial Registration: Clinical Trial Registry–India identifier: CTRI/2023/09/057998
Prim Care Companion CNS Disord 2026;28(3):25m04143
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Alcohol use is influenced by cultural norms and neurobiological factors, involving a balance between its adverse consequences and rewarding effects, such as euphoria and anxiety relief.1 The transition from occasional drinking to dependence is driven by adaptive changes, including downregulation of dopamine and γ-aminobutyric acid (GABA) systems, persistent glutamate hyperactivity, and dysregulation of brain stress pathways.2
Alcohol use disorder (AUD) is frequently accompanied by anxiety and depression, affecting 20%–40% of individuals globally. These comorbid conditions significantly increase the overall burden of illness. In India, depression is reported in 30%–40% of people with AUD, consistent with global estimates.3
Treatment for alcohol dependence syndrome usually starts with detoxification. As the gold standard for treating alcohol withdrawal, benzodiazepines are a mainstay of therapeutic treatment since they have been shown to effectively reduce symptoms including anxiety and seizures.4 Benzodiazepines are effective for managing anxiety disorders and should be used judiciously after evaluating risk factors such as substance use history, concurrent opioid or alcohol use, older age, fall risk, and cognitive impairment.5 They may also be particularly helpful in individuals with depression and comorbid anxiety or insomnia, where they can alleviate anxiety and sleep disturbances.6
Lorazepam is a short-acting benzodiazepine (half-life of 10–20 hours) without active metabolites, whereas diazepam is long-acting (half-life of 20–50 hours) and is metabolized in the liver to active metabolites via cytochrome P450, family 3, subfamily A, and member 4 pathways. Both have similar mechanisms, food-independent absorption, and contraindications but differ in metabolism and duration of action.7
Two main strategies are used for managing alcohol withdrawal with benzodiazepines: the loading method and the symptom-triggered approach.8 The loading method uses long-acting benzodiazepines to gradually reduce withdrawal symptoms but may cause excessive sedation, respiratory depression, and longer hospital stays.8,9 In contrast, the symptom-triggered approach uses short-acting benzodiazepines, adjusting doses according to clinical symptoms, commonly assessed with the Clinical Institute Withdrawal Assessment for Alcohol–Revised (CIWA-Ar) scale.10 While concerns include breakthrough symptoms and potential benzodiazepine dependence, this approach is noted for its safety, effectiveness, and shorter treatment duration.8,10
A study across 3 Vancouver emergency departments (2015–2018) compared lorazepam (n = 394) and diazepam (n = 504) for acute alcohol withdrawal in 1,055 patients, excluding those with seizures or acute medical illness. Outcomes—including hospital admissions, in-ED seizures, and 1-week return visits—were similar between groups.11
A retrospective cohort of 191 ICU patients with severe alcohol withdrawal compared injectable diazepam (n=89) and lorazepam (n = 102), each receiving ≥12 lorazepam -equivalent units in 24 hours. Both maintained target CIWA-Ar scores with comparable total doses, but diazepam was significantly more expensive. The study concluded that although both are effective, lorazepam may be preferred due to lower cost.12 A few studies compared lorazepam and chlordiazepoxide in treatment of alcohol withdrawal and prevention of delirium tremens in which both drugs were found to be equally effective.13,14
Despite the long-standing use of benzodiazepines for alcohol detoxification, there remains limited high-quality, head-to-head evidence comparing lorazepam and diazepam, particularly regarding the speed of withdrawal symptom resolution. Although both are widely used, direct data on how quickly each alleviates symptoms are scarce, and their comparative effects on co-occurring anxiety and depression are not well studied. Existing retrospective and small-scale studies suggest similar efficacy, but the evidence is insufficient to guide clear clinical decisions. Given the high prevalence of affective symptoms during withdrawal and ongoing concerns about benzodiazepine dependence, this study aims to address a key gap and support more individualized treatment selection in alcohol dependence syndrome.
METHODS
Description
A total of 80 consecutive patients diagnosed with alcohol dependence syndrome (International Classification of Diseases, Eleventh Revision)15 were screened. Of 80 patients, 11 did not provide consent. Of the 69 patients who were randomized, 9 were excluded during the follow-up period: 4 due to loss to follow-up and 5 due to resumption of dependent alcohol use (syndromal relapse). These exclusions occurred after completion of detoxification. The dropouts were evenly distributed between the treatment groups (lorazepam = 4, diazepam = 5), resulting in a final sample of 60 patients (30 per group) for analysis.
Male patients in the age group of ≥25 years, CIWA-Ar score <15, were admitted to the substance use disorder ward of the psychiatry department of a tertiary care teaching hospital in Northern India. Patients with epilepsy, dependence on other substances except nicotine and caffeine, past history of complicated withdrawals, current intoxication, comorbid active psychotic illness, and any acute medical or surgical illness, as well as actively suicidal patients were excluded from the study.
A semistructured proforma was used to record sociodemographic and clinical data. Baseline investigations included complete hemogram, liver function tests, serum electrolytes and renal function tests, lipid profile, and electrocardiogram. At baseline, the CIWA-Ar16 and Severity of Alcohol Dependence Questionnaire (SADQ),17 Hamilton Anxiety Rating Scale (HAM-A),18 and Hamilton Depression Rating Scale (HAM-D)19 were administered. Patients were randomly assigned to 2 groups, and detoxification was done using either lorazepam or diazepam in a symptom-triggered regimen: lorazepam (4 mg/day initiation; 3–4 divided dosages and 1 mg/day titration) and diazepam (10 mg/day initiation; 1–2 dosages per day and 5 mg/day titration) orally, adjusted as per CIWA-Ar scores and side effect profiles. CIWA-Ar scores were recorded daily before the morning dose to monitor withdrawal symptoms by the principal investigator (S.S.). The HAM-A and HAM-D were readministered after detoxification to assess anxiety and depressive symptoms. Once 50% relief in withdrawal symptoms was noted, the respective benzodiazepines were downtitrated. Efforts were made to keep the benzodiazepines at minimal doses, and they were gradually stopped over 3–4 weeks. No additional SSRIs were prescribed. All patients were offered baclofen (10 mg/day) after detoxification. In case of baclofen use, dosing was uptitrated by 10 mg every 3 days based on cravings unless adverse effects occurred, in which case adjustments were slower (10 mg every 4–10 days or 5-mg increments).20
Further, patients were followed up regularly until week 12 of the study (including treatment with baclofen) to ensure compliance and abstinence. During this time, if patients resorted to alcohol use again apart from dependent use, the alcohol use pattern was recorded at follow-ups. Moderate drinking or nondependent use of alcohol was referred to as <14 drinks per week.3 Intermittent users were patients who consumed <20% of their usual intake per day, not on 3 consecutive days, and not having any socio-occupational dysfunction due to alcohol use in the past week.21 For the purpose of this study, if patients had not consumed alcohol in 2 weeks prior to the date of follow-up, it was considered as abstinence. If patients resumed drinking patterns as before they sought treatment, it was referred to as syndromal relapse, and they were then excluded from the study. Assessment and comparison of anxiety and depression at baseline, after detoxification, and after 12 weeks was done with the HAM-A and HAM-D.
Ethical Considerations
The purpose and design of the study were explained to the patient in a language they understood. The patient had the right to withdraw from the study at any time without providing a reason. The confidentiality of the information gathered was maintained. The study was conducted in accordance with the defined guidelines of the Central Ethics Committee and the principles enunciated in the Declaration of Helsinki. The study was approved by the Institutional Ethics Committee (GMCH/IEC/2023/1045R) and registered with the Clinical Trial Registry–India (identifier: CTRI/2023/09/057998).
Statistical Analysis
Data were coded and recorded in Microsoft Excel. SPSS v2322 was used for data analysis. Descriptive statistics were elaborated in the form of means/SDs for continuous variables and frequencies/percentages for categorical variables. Association between 2 categorical variables was explored using χ2 test. In case the expected frequency in the contingency tables was found to be <5 for >25% of the cells, Fisher exact test was used instead. Associations between a continuous variable and a categorical variable with 2 groups were assessed using the independent sample t-test. A P value <.05 was considered statistically significant and < .001 was considered highly significant.
RESULTS
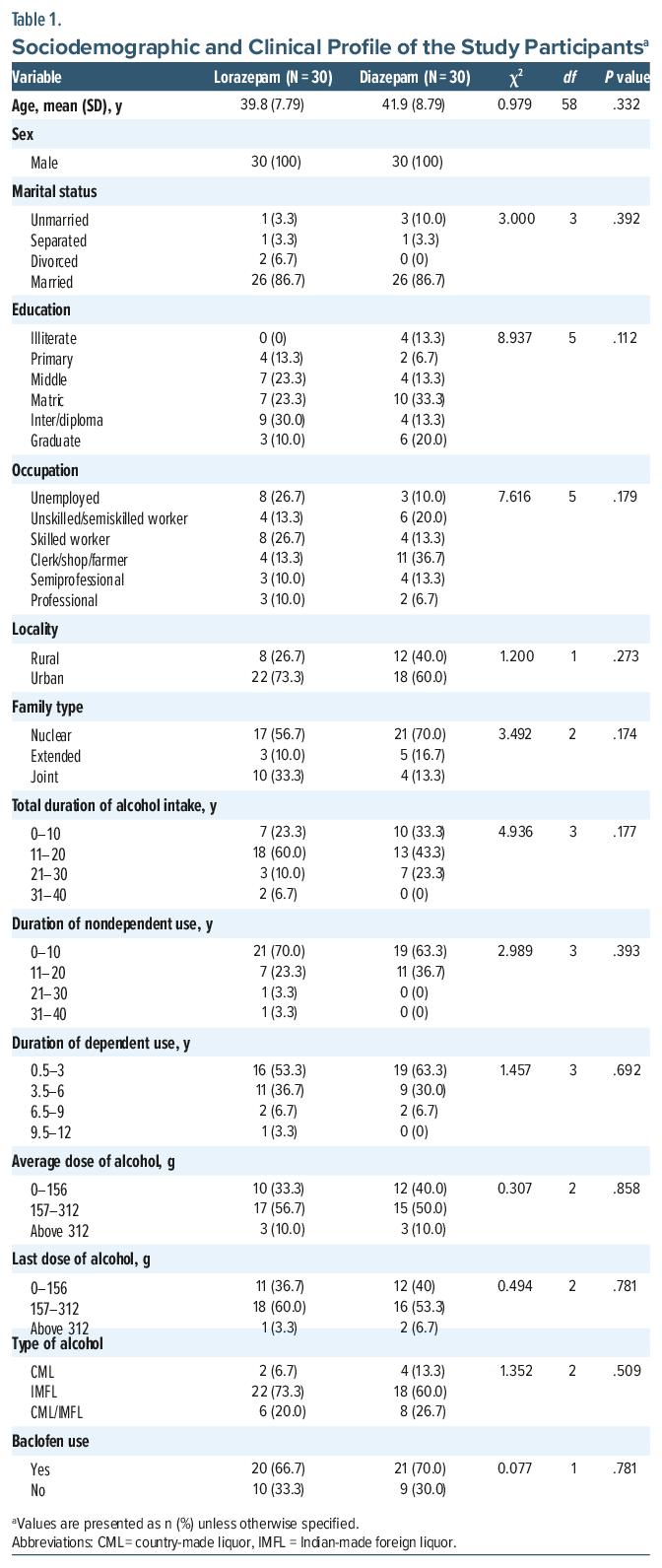
Sociodemographic and Clinical Profile The 2 treatment groups were comparable in sociodemographic and alcohol-use characteristics. Participants were predominantly middle-aged, married males, largely from urban backgrounds and nuclear families, with similar levels of educational attainment and occupational distribution. Alcohol-use patterns were alike across groups, including total duration of intake, progression to dependence, and duration of dependent use. Average and recent alcohol consumption, type of alcohol consumed, and postdetoxification baclofen use were similarly distributed, indicating a homogeneous baseline sample as shown in Table 1.
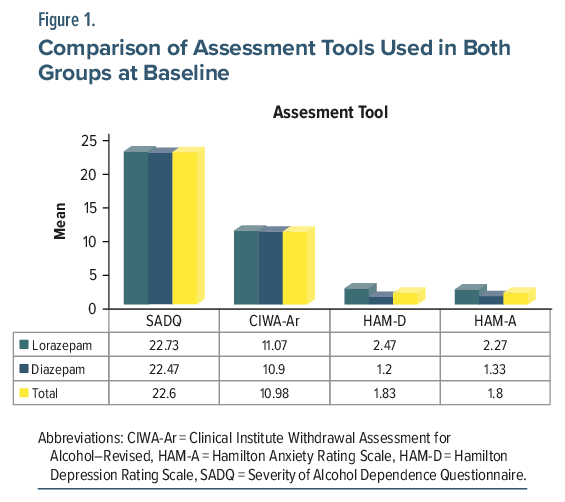
SADQ scores were comparable between groups, with means of 22.73 (SD = 5.74) in the lorazepam group and 22.47 (SD = 3.75) in the diazepam group (P = .832), indicating moderate dependence in both groups. CIWA Ar scores were also similar (P = .795), with means of 11.07 (SD = 2.7) and 10.9 (SD = 2.22), respectively, reflecting comparable withdrawal severity. Depression severity (HAM-D) was slightly higher in the lorazepam group (mean = 2.47, SD = 3.94) than in the diazepam group (mean = 1.2, SD = 1.3), though not statistically significant (P = .122). Anxiety scores (HAM-A) were likewise higher in the lorazepam group (mean = 2.27, SD = 2.69) compared to diazepam (mean = 1.33, SD = 1.84) but were not statistically significant (P = .100). Overall, both groups demonstrated comparable levels of dependence, withdrawal severity, depression, and anxiety as shown in Figure 1.
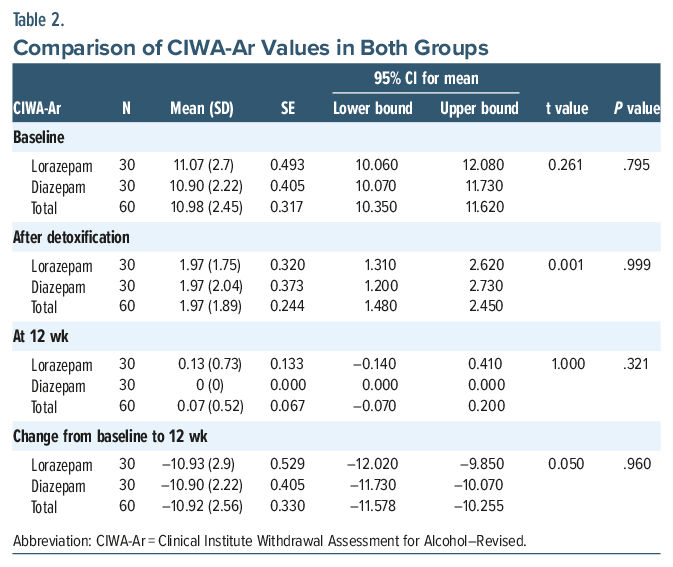
CIWA-Ar scores showed a significant decline from baseline to 12 weeks in both groups, with no significant differences between them. Baseline scores were similar (lorazepam: mean = 11.07; diazepam: mean = 10.9; P = .795). After detoxification, scores reduced markedly in both groups (mean = 1.97; P = .999). By 12 weeks, residual symptoms were minimal (lorazepam: mean = 0.13; diazepam: mean = 0; P = .321). The overall reduction in scores was nearly identical (–10.93 vs –10.9; P = .960), indicating both drugs were equally effective in resolving withdrawal symptoms over time as shown in Table 2.
Symptom control during the withdrawal phase was assessed using daily CIWA-Ar scores under a symptom-triggered regimen. Both treatment groups demonstrated comparable dose requirements and similar time to achieve more than 50% reduction in withdrawal symptoms, indicating no significant difference in the need for dose augmentation during detoxification.
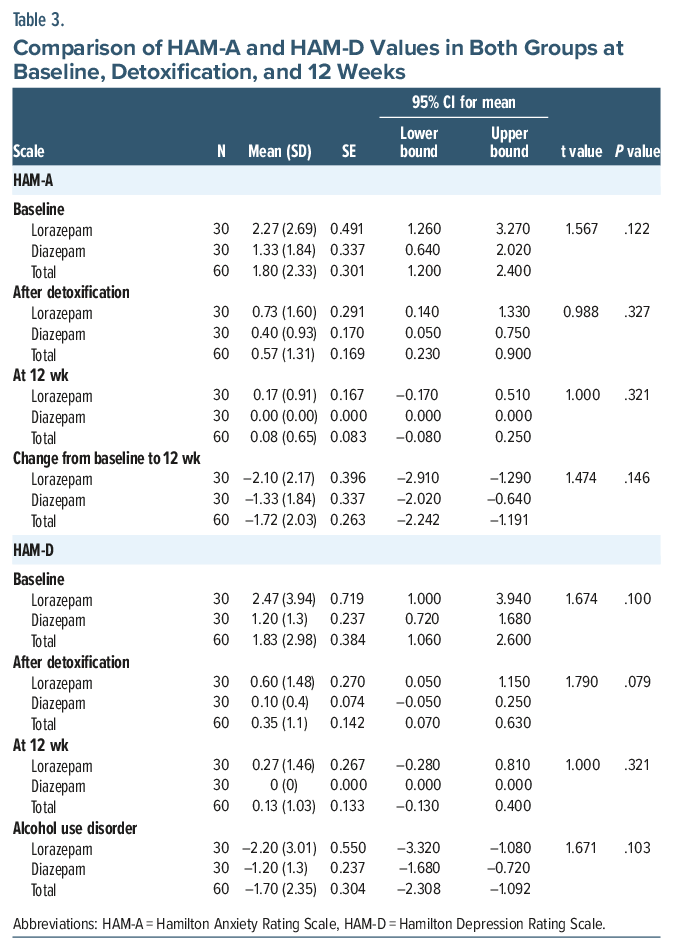
HAM-A scores declined in both groups over 12 weeks, with no statistically significant differences. Baseline anxiety was higher in the lorazepam group (mean = 2.27) than in the diazepam group (mean = 1.33; P = .122). In the lorazepam and diazepam groups, postdetoxification scores decreased to 0.73 and 0.4, respectively (P = .327), and 12-week scores decreased to 0.17 and 0, respectively (P = .321). The overall reduction was slightly greater in the lorazepam group (–2.1 vs –1.33; P = .146), indicating comparable effectiveness in reducing anxiety.
Similarly, HAM-D scores declined in both groups, with no significant differences. Baseline depression was slightly higher in the lorazepam group (mean=2.47) compared to diazepam (mean=1.2; P=.100). In the lorazepam and diazepam groups, postdetoxification scores declined to 0.6 and 0.1, respectively (P=.079), and 12-week scores decreased to 0.27 and 0, respectively (P=.321). The reduction was greater in the lorazepam group (–2.2 vs. –1.2; P =.103), again suggesting similar effectiveness in reducing depressive symptoms as shown in Table 3.
The average daily dose was 5.56 mg/day (SD = 1.16) for lorazepam and 17.14 mg/day (SD = 4.81) for diazepam, reflecting the differing dose ranges typically used in alcohol withdrawal management. Both drugs were equally effective in achieving a 50% reduction in withdrawal symptoms, with no significant difference between groups (P = .214). Time to >50% symptom reduction was slightly shorter with diazepam (4.6 vs. 4.97 days; P = .241).
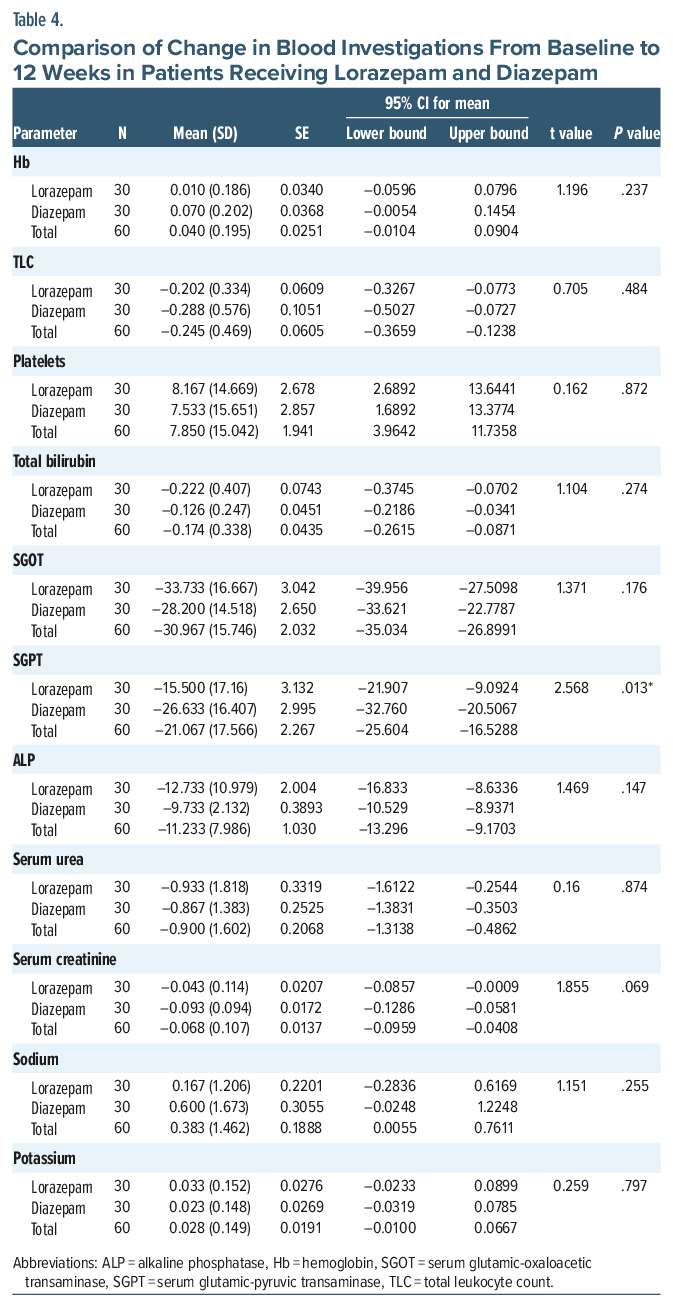
The 12-week comparison of lorazepam and diazepam showed similar effects across most physiological parameters. Serum glutamic-pyruvic transaminase (SGPT) decreased significantly more with diazepam (P = .013). Overall, both drugs produced similar physiological effects, with diazepam having a stronger influence on SGPT levels as shown in Table 4.
DISCUSSION
This study compared the clinical efficacy of lorazepam and diazepam in managing alcohol withdrawal and associated anxiety and depression. It was a prospective, randomized interventional study, with participants predominantly middle-aged males, consistent with epidemiologic patterns in alcohol dependence. The findings support existing evidence that both medications are effective in symptom-triggered detoxification, providing comparable improvement in withdrawal symptoms and related affective disturbances.
The participants (Table 1) were primarily middle-aged married males, consistent with sociodemographic profiles reported by Vignesh et al23 and Gupta et al.24 Educational levels varied, aligning with Pradeep et al,25 although Vignesh et al23 reported a stronger association between lower education and dependence. Occupational status, residence, and family type also corresponded with findings from Vignesh et al.23 Most participants had consumed alcohol for 11–20 years, similar to Manning et al,26 but shorter than the 44-year duration observed by Munro et al27 likely due to differing age profiles. The durations of nondependent and dependent drinking phases were shorter than those reported by Pitel et al,28 Zinn et al,29 and Brion et al,30 which may reflect genetic variations (eg, alcohol dehydrogenase 1B and aldehyde dehydrogenase 2 polymorphisms) influencing vulnerability.31 Indian-made foreign liquor was the most-consumed alcohol type, likely due to urban accessibility. Baclofen was prescribed in most cases, supporting its documented effectiveness in reducing cravings by Rozatkar et al.21
In the index study, baseline comparisons of CIWA-Ar, SADQ, HAM-A, and HAM-D scores between the lorazepam and diazepam groups (Figure 1) showed no statistically significant differences, indicating that both groups had comparable levels of alcohol dependence, withdrawal severity, anxiety, and depression at the outset.
The improvement in CIWA-Ar scores from baseline to detoxification and at the 12-week follow-up (Table 2) was similar in both the lorazepam and diazepam groups, indicating significant symptom relief without a meaningful difference between them. Once withdrawal symptoms had reduced by 50%, benzodiazepines were gradually tapered, and their use did not extend beyond 3–4 weeks. These findings suggest that both medications were equally effective in alleviating withdrawal symptoms over time, consistent with previous studies reporting comparable efficacy of lorazepam and diazepam in alcohol withdrawal management.10,11,32,33
In a study by Ritson and Chick,34 both lorazepam and diazepam were found to be equally effective in cases of alcohol withdrawal, but diazepam resulted in a smoother withdrawal resolution. However, no significant difference with reference to this was noted in our study.
In this study, the lorazepam group demonstrated a greater overall reduction in HAM-A scores from baseline to 12 weeks compared to the diazepam group (Table 3), though the difference was not statistically significant. This indicates that both medications were effective in reducing anxiety over time, yielding comparable outcomes. These findings are consistent with earlier studies reporting similar anxiolytic efficacy for both agents.35,36
As per the current study, the lorazepam group showed a greater reduction in HAM-D scores from baseline to 12 weeks than the diazepam group (Table 3), though the difference was not statistically significant. This finding suggests that both medications were similarly effective in reducing depressive symptoms over time, indicating that an additional SSRI may not be necessary for mild comorbid anxiety and depression in alcohol dependence syndrome.
In a study by Zung et al,36 patients were divided into 2 groups—those with predominant depression and those with predominant anxiety. In the predominantly depressive group, all treatments (prazepam, lorazepam, diazepam, and placebo) reduced both anxiety and depression. However, in the predominantly anxiety group, only prazepam and placebo improved both symptoms, while diazepam and lorazepam reduced anxiety but had minimal effect on depression. The findings of the present study align with this pattern, as participants had higher anxiety and lower depressive symptoms, which may explain the similar trends observed in HAM-A and HAM-D scores.
In this study, there was no statistically significant difference in the number of days required to achieve 50% resolution of withdrawal symptoms with either drug, although diazepam showed a slightly faster reduction. The average daily dose ratio of lorazepam to diazepam was approximately 1:3, whereas the commonly accepted equivalence suggests 2 mg lorazepam ≈10 mg diazepam (1:5). This variation may be attributed to differences in bioavailability and individual drug metabolism. To the best of our knowledge, there is no available literature on comparison of average daily dose of both drugs and time taken for resolution of withdrawal symptoms.
At baseline, hematologic parameters were comparable between the lorazepam and diazepam groups, indicating similar clinical and biochemical profiles prior to intervention. Over the 12-week abstinence period, most biochemical parameters remained comparable, except for SGPT, which showed a significantly greater reduction in the diazepam group (P = .013; Table 4). Although diazepam is generally avoided in advanced liver disease due to its active metabolites and risk of hepatic encephalopathy, while lorazepam is glucuronidated and lacks active metabolites, the observed SGPT change may reflect individual hepatic enzyme variability and adaptive metabolic shifts during abstinence. Further research is needed to clarify this finding, as other liver function parameters did not show similar trends.
This study has several strengths, including its randomized design, use of a symptom-triggered detoxification protocol, validated assessment tools, and a 12-week follow-up that allowed evaluation of both withdrawal symptoms and comorbid anxiety and depression. However, limitations include a small, male-only sample and single-center setting, which limit generalizability. Therefore, the findings should be interpreted as preliminary, and larger multicentric studies including female participants are required to validate these results. The absence of a nonmedicated control group prevents distinguishing medication effects from natural recovery. Although neither lorazepam nor diazepam was continued beyond 4 weeks, occasional as-needed use cannot be excluded. The effect of baclofen on craving was also not assessed. The near-uniform use of baclofen during follow-up limited separate analysis of its independent effect on anxiety and depressive symptoms. Duration of hospital admission was not formally evaluated as an outcome measure in this study and may represent an important clinical variable for future research comparing benzodiazepines in alcohol withdrawal management. Additionally, the 3-month follow-up reflects short-term outcomes and may not capture longer-term recovery patterns.
CONCLUSION
This study indicates that symptom-triggered regimens of lorazepam and diazepam are comparably effective in managing withdrawal symptoms in individuals with moderate level of alcohol dependence syndrome. Although the lorazepam group showed slightly greater reductions in anxiety and depression over 12 weeks and diazepam demonstrated a marginally faster >50% reduction in CIWA-Ar scores, these differences were not statistically significant and do not support the preferential use of either agent. In the absence of statistically significant differences, selection of either agent may be guided by clinical context, pharmacokinetic considerations, patient characteristics, and clinician preference. Diazepam, however, produced a statistically significant reduction in SGPT levels. Overall, both medications were effective for detoxification and provided similar outcomes in alleviating withdrawal, anxiety, and depressive symptoms. Nevertheless, the modest sample size and limited participant diversity warrant further studies to validate these results in broader clinical populations.
Article Information
Published Online: May 26, 2026. https://doi.org/10.4088/PCC.25m04143
© 2026 Physicians Postgraduate Press, Inc.
Submitted: November 20, 2025; accepted February 2, 2026.
To Cite: Sharma S, Sidana A, Mehta S, et al. Lorazepam versus diazepam in alcohol dependence syndrome: which is better? Prim Care Companion CNS Disord 2026;28(3):25m04143.
Author Affiliations: Department of Psychiatry, Government Medical College and Hospital, Chandigarh (Sharma, Sidana, Mehta); Department of Computer Science Engineering, Thapar Institute of Engineering and Technology, Patiala, Punjab (Kaur).
Corresponding Author: Ajeet Sidana, MD, Department of Psychiatry, Government Medical College and Hospital, Chandigarh, India ([email protected]).
Previous Presentation: The study was presented at the Golden Jubilee Conference of Indian Psychiatric Society-North Zone; October 11–12, 2025; Chandigarh, India.
Clinical Points
- Both lorazepam and diazepam led to more than 50% reduction in Clinical Institute Withdrawal Assessment for Alcohol–Revised scores within 5 days of initiation of treatment in alcohol dependence syndrome.
- Lorazepam showed numerically greater reduction in depressive and anxiety symptoms than diazepam, though differences were not statistically significant.
- Diazepam’s longer half-life may offer practical advantages in certain clinical situations, including smoother withdrawal in selected patients.
- Diazepam leads to better reduction in serum glutamic-pyruvic transaminase value.
References (36)

- Becker HC. Alcohol dependence, withdrawal and relapse. Alcohol Res Health. 2008;31(4):348–361. PubMed
- Roberto M, Gilpin NW, Siggins GR. The central amygdala and alcohol: role of γ-aminobutyric acid, glutamate, and neuropeptides. Cold Spring Harb Perspect Med. 2012;2(12):a012195. PubMed CrossRef
- Understanding Alcohol Drinking Patterns. National Institute on Alcohol Abuse and Alcoholism; Bethesda, MD; 2023. https://www.niaaa.nih.gov/alcohols-effects-health/alcohol-drinking-patterns
- Ozdemir V, Bremner KE, Naranjo CA. Treatment of alcohol withdrawal syndrome. Ann Med. 1994;26(2):101–105. PubMed CrossRef
- Hirschtritt ME, Olfson M, Kroenke K. Balancing the risks and benefits of benzodiazepines. JAMA. 2021;325(4):347–348. PubMed CrossRef
- de Cates A, De Giorgi R. Antidepressants plus benzodiazepines in major depressive disorder: a clinical dilemma with no recent answers from research. BJPsych Adv. 2020;26(6):321–326. PubMed CrossRef
- Stahl SM, Grady MM, Muntner N. Stahl’s Essential Psychopharmacology: Prescriber’s Guide Antidepressants. Cambridge, United Kingdom: Cambridge University Press; 2017.
- Maldonado JR, DiMartini A, Owen J. Psychopharmacological treatment of substance use disorders in the medically ill. In: Levenson JL, Ferrando SJ, eds. Clinical Manual of Psychopharmacology in the Medically Ill. American Psychiatric Publishing;2010:537–555.
- Sellers EM, Naranjo CA, Harrison M, et al. Diazepam loading: simplified treatment of alcohol withdrawal. Clin Pharmacol Ther. 1983;34:822–826. PubMed CrossRef
- McKay A, Koranda A, Axen D. Using a symptom-triggered approach to manage patients in acute alcohol withdrawal. Medsurg Nurs. 2004;13(1):15–20. PubMed
- Scheuermeyer FX, Miles I, Lane DJ, et al. Lorazepam versus diazepam in the management of emergency department patients with alcohol withdrawal. Ann Emerg Med. 2020;76(6):774–781. PubMed CrossRef
- Brickel KH, Hodge EK, Zavgorodnyaya D, et al. A comparison of injectable diazepam and lorazepam in the goal-directed management of severe alcohol withdrawal. Ann Pharmacother. 2024;58(5):453–460. PubMed CrossRef
- Kumar CN, Andrade C, Murthy P. A randomized, double-blind comparison of lorazepam and chlordiazepoxide in patients with uncomplicated alcohol withdrawal. J Stud Alcohol Drugs. 2009;70(3):467–474. PubMed CrossRef
- March KL, Twilla JD, Reaves AB, et al. Lorazepam versus chlordiazepoxide for the treatment of alcohol withdrawal syndrome and prevention of delirium tremens in general medicine ward patients. Alcohol. 2019;81:56–60. PubMed CrossRef
- World Health Organization. International Classification of Diseases and Related Health Problems. 11th revision. Geneva: World Health Organization; 2019
- Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised Clinical Institute Withdrawal Assessment for Alcohol Scale (CIWA-Ar). Br J Addict. 1989;84(11):1353–1357. PubMed CrossRef
- Stockwell T, Sitharthan T, McGrath D, et al. The measurement of alcohol dependence and impaired control in community samples. Addiction. 1994;89(2):167–174. PubMed CrossRef
- Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. PubMed CrossRef
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56–62. PubMed CrossRef
- Imbert S, Blaise S, Bérard J, et al. A prescription guide for baclofen in alcohol use disorder- for use by physicians and patients. J Addict Med Ther Sci. 2017;3:32–41.
- Rozatkar AR, Kapoor A, Sidana A, et al. Clinical experience of baclofen in alcohol dependence: a chart review. Ind Psychiatry J. 2016;25(1):11–16. PubMed CrossRef
- IBM Corp. IBM SPSS Statistics for Windows, Version 23.0. IBM Corp; 2015.
- Vignesh BT, Singh AK, Mohan SK, et al. Association between socio-demographics and alcohol dependence among individuals living in an Indian setting. Glob J Health Sci. 2014;6(3):16–26. PubMed CrossRef
- Gupta R, Sinha S, Khanna P, et al. Marital status and alcohol dependence: a clinical perspective. Indian J Psychiatry. 2020;62:297–304.
- Pradeep RJ, Banu S, Ashok MV. Severity of alcoholism in Indian males: correlation with age of onset and family history of alcoholism. Indian J Psychiatry. 2010;52:243–249. PubMed CrossRef
- Manning V, Wanigaratne S, Best D, et al. Changes in neuropsychological functioning during alcohol detoxification. Eur Addict Res. 2008;14(4):226–233. PubMed CrossRef
- Munro CA, Saxton J, Butters MA. The neuropsychological consequences of abstinence among older alcoholics: a cross-sectional study. Alcohol Clin Exp Res. 2000;24(10):1510–1516. PubMed CrossRef
- Pitel AL, Rivier J, Beaunieux H, et al. Changes in the episodic memory and executive functions of abstinent and relapsed alcoholics over a 6-month period. Alcohol Clin Exp Res. 2009;33(3):490–498. PubMed CrossRef
- Zinn S, Stein R, Swartzwelder HS. Executive functioning early in abstinence from alcohol. Alcohol Clin Exp Res. 2004;28(9):1338–1346. PubMed CrossRef
- Brion M, D’Hondt F, Pitel AL, et al. Executive functions in alcohol-dependence: a theoretically grounded and integrative exploration. Drug Alcohol Depend. 2017;177:39–47.
- Edenberg HJ. The genetics of alcohol metabolism: Role of alcohol dehydrogenase and aldehyde dehydrogenase variants. Alcohol Res Health. 2007;30(1):5–13. PubMed
- Levine AR, Thanikonda V, Mueller J, et al. Front-loaded diazepam versus lorazepam for treatment of alcohol withdrawal agitated delirium. Am J Emerg Med. 2021;44:415–418. PubMed CrossRef
- Miller WCJr, McCurdy L. A double-blind comparison of the efficacy and safety of lorazepam and diazepam in the treatment of the acute alcohol withdrawal syndrome. Clin Ther. 1984;6(3):364–371. PubMed
- Ritson B, Chick J. Comparison of two benzodiazepines in the treatment of alcohol withdrawal: effects on symptoms and cognitive recovery. Drug Alcohol Depend. 1986;18(4):329–334. PubMed CrossRef
- Itoh H, Ohtsuka N, Kamishima K, et al. A comparative clinical study for the evaluation of antianxiety agents, (lorazepam, diazepam and placebo), in neurosis. Folia Psychiatr Neurol Jpn. 1977;31(1):25–35. PubMed CrossRef
- Zung WW, Daniel JT Jr, King RE, et al. A comparison of prazepam, diazepam, lorazepam and placebo in anxious outpatients in non-psychiatric private practices. J Clin Psychiatry. 1981;42(7):280–284. PubMed
Please sign in or purchase this PDF for $40.




