Abstract
Objective: Cardiovascular disease (CVD) and posttraumatic stress disorder (PTSD) are prevalent and disabling conditions among older US veterans. Both are independently associated with poor physical, mental, and functional outcomes, but little is known about the combined burden. This study aims to examine the prevalence, risk correlates, health comorbidities, and functional outcomes of comorbid CVD+PTSD in older US veterans.
Methods: Data were analyzed from 3,001 US veterans aged 60 years and older who participated in the 2019–2020 National Health and Resilience in Veterans Study. Self-reported CVD, PTSD, health comorbidities, and functional outcomes were examined using weighted bivariate and multivariable analyses.
Results: A total of 23.1% of veterans had CVD only, 5.5% PTSD only, and 2.2% comorbid CVD+PTSD. Veterans with CVD+PTSD were more likely to report combat exposure, childhood adversity, and greater lifetime trauma compared to other groups. Relative to controls, they had particularly elevated odds of major depressive disorder (MDD), generalized anxiety disorder (GAD), cognitive disorder (ie, mild cognitive impairment, dementia, or Alzheimer disease), sleep disorder, and concussion/traumatic brain injury (TBI; odds ratios [ORs] = 4.78–13.27). Compared to CVD-only veterans, those with CVD+PTSD had higher odds of GAD, MDD, cognitive disorder, sleep disorder, suicidal ideation, and chronic pain (ORs = 1.89–9.64). Relative to PTSD-only veterans, they had greater odds of kidney disease, concussion/TBI, MDD, and sleep disorder (ORs = 2.67–4.85). Veterans with CVD+PTSD also showed moderately greater impairments in psychosocial and cognitive functioning compared to single-diagnosis groups (d’s = 0.50–0.66).
Conclusions: Older veterans with comorbid CVD+PTSD have a markedly elevated burden of health and functional difficulties, underscoring the importance of integrated, trauma-informed care to improve outcomes in this high-risk population.
Prim Care Companion CNS Disord 2026;28(4):26m04187
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Cardiovascular disease (CVD) is a leading cause of morbidity, mortality, and functional decline in older adults.1,2 This burden is particularly pronounced among US veterans, with 25.2% of those aged 60 years and older reporting having been diagnosed with CVD (ie, heart disease, heart attack, and/or stroke),3 and numerous studies documenting higher rates of CVD in veterans compared with nonveterans.4–8 Beyond its prevalence, CVD often co-occurs with a wide range of physical and mental health comorbidities. Veterans with CVD are more likely to experience physical and mental health conditions such as arthritis, cancer, kidney disease, mild cognitive impairment, dementia, and Alzheimer disease, as well as mood and anxiety disorders.3 CVD is also linked to cognitive difficulties, including impairments in memory, attention, and executive functioning.9
In parallel, posttraumatic stress disorder (PTSD) is highly prevalent in the veteran population.10 Nationally representative estimates indicate a lifetime prevalence of 9.4% and a past-month prevalence of 5.0%.10 Similar to the burden observed with CVD, PTSD is associated with numerous physical and mental health comorbidities, including chronic pain, sleep disorders, substance use disorders (SUDs), and suicidal thoughts and behaviors.11,12 PTSD is also linked to decrements in physical, mental, and social functioning and reduced quality of life.13–15
CVD and PTSD are strongly interrelated and often co-occur.16,17 Accumulating research suggests cumulative health effects when these conditions overlap. For example, in a cohort of Vietnam-deployed veterans surveyed 50 years postwar, PTSD was associated with a higher likelihood of CVD, and those with CVD reported significantly more comorbid conditions, including arthritis, sleep apnea, emphysema, and asthma.18 More broadly, multimorbidity in veterans is linked to greater symptom burden and reduced functional independence and quality of life.19 Collectively, these findings suggest that comorbid CVD and PTSD (CVD+PTSD) may exacerbate physical and mental health burden and associated functional impairments. However, the scope of this impact remains poorly understood, particularly in nationally representative veteran samples. A comprehensive evaluation of the combined impacts of CVD and PTSD on older veterans’ health and functioning is essential to informing integrated care models for this population.
Although prior research has largely examined CVD and PTSD separately, relatively few studies have investigated their combined effects. Important gaps remain regarding which veterans may be at greater risk of developing CVD+PTSD and how this comorbidity may influence physical, mental, and functional outcomes in veterans. To address these gaps, the current study aimed to (1) estimate the prevalence of CVD, PTSD, and CVD+PTSD among a nationally representative sample of US veterans aged 60 years and older; (2) identify sociodemographic, military, trauma-related, and lifetime risk correlates associated with CVD+PTSD relative to controls and to single-diagnosis groups (CVD only and PTSD only); (3) evaluate physical and mental health comorbidities associated with CVD+PTSD relative to controls and single-diagnosis groups; and (4) assess functional consequences associated with CVD+PTSD compared with single-diagnosis groups.
METHODS
Sample
The 2019–2020 National Health and Resilience in Veterans Study surveyed a nationally representative sample of 4,069 US veterans. Of these, 3,001 participants were aged 60 years or older. The sample was drawn from KnowledgePanel, a probability-based, online, nonvolunteer survey panel of a nationally representative sample of US adults. Panel recruitment relies on random sampling methods, originally conducted via telephone and now primarily through postal mail. The sampling strategy uses dual sampling frames that include both listed and unlisted telephone numbers, telephone and nontelephone households, and cellphone-only households, as well as households with and without internet access. Further methodological details are available elsewhere.10 Participants completed an anonymous, web-based survey, with a median completion time of 49 minutes. To enable generalizability of results to the US veteran population, poststratification weights were applied based on benchmark data from the August 2019 Veterans Supplement of the Current Population Survey.20 All procedures were approved by the Human Subjects Committee of the VA Connecticut Healthcare System, and all participants provided electronic informed consent.
Measures
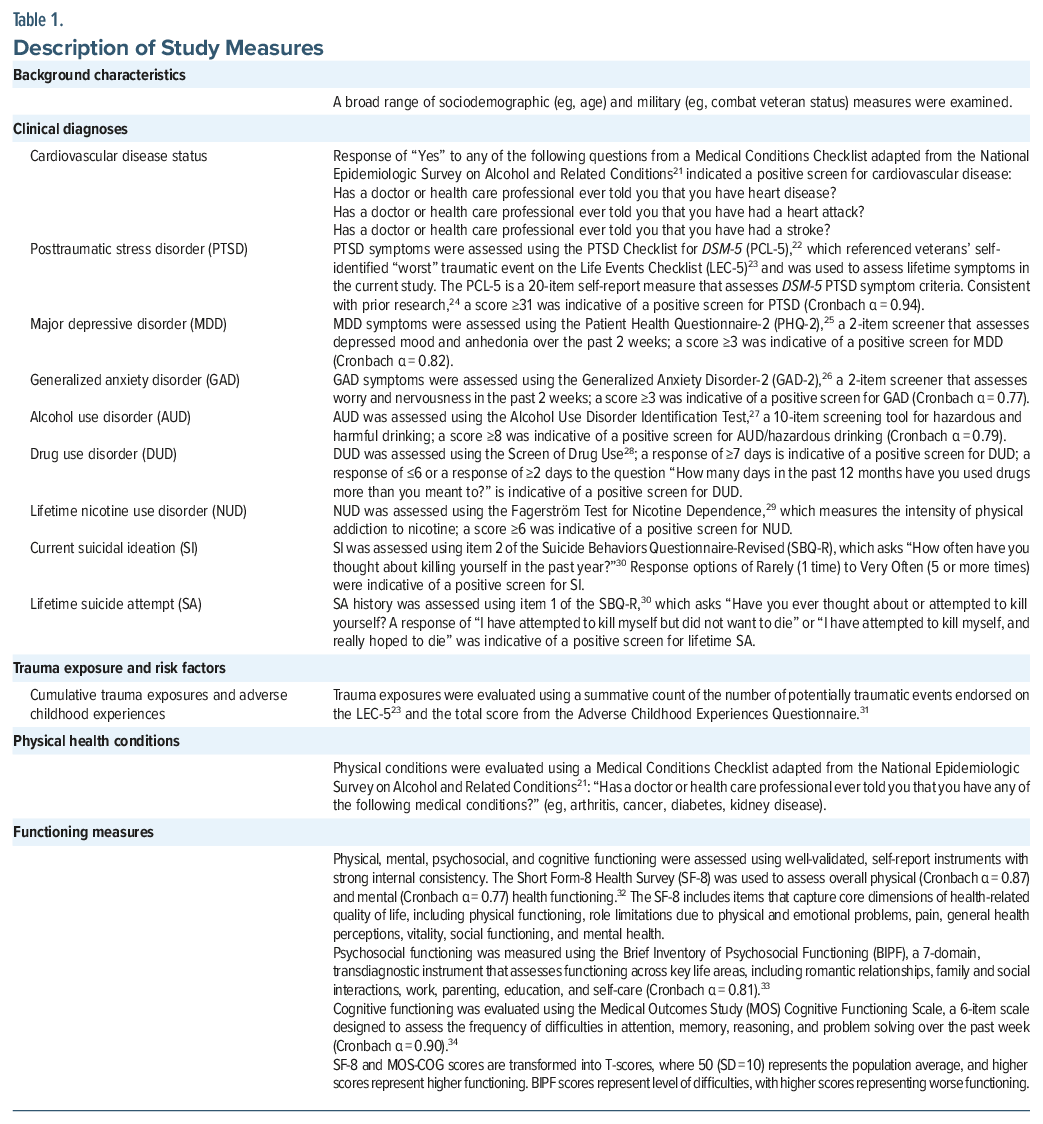
Key measures included self-reported diagnoses of CVD and PTSD, as well as sociodemographic, trauma-related, physical health, psychiatric, and functional variables. A complete description of all study measures is provided in Table 1.
Data Analysis
Data analysis proceeded in 4 steps. First, descriptive statistics were computed to estimate the prevalence of veterans with (1) neither CVD nor PTSD (controls); (2) CVD only (CVD but no PTSD); (3) PTSD only (PTSD but no CVD); and (4) CVD+PTSD. Second, weighted 1-way analyses of variance and χ2 analyses were conducted to compare these subgroups with respect to sociodemographic characteristics, military service variables, and lifetime risk factors. Third, a series of binary multivariable logistic regression analyses was conducted to identify independent correlates of CVD+PTSD, and to assess associations between CVD and PTSD groups and measures of physical and mental health disorders. Finally, a series of weighted multivariable analyses of covariances was conducted to examine associations between CVD and PTSD groups and measures of functioning. Variables that differed between groups in bivariate analyses were adjusted for in all multivariable analyses. To account for multiple comparisons, Bonferroni-corrected significance levels were used. Cohen d was calculated for effect size estimations using means, SEs, and sample sizes, where small, medium, and large effects were quantified as 0.20, 0.50, and 0.80, respectively.35,36
RESULTS
Sample Characteristics
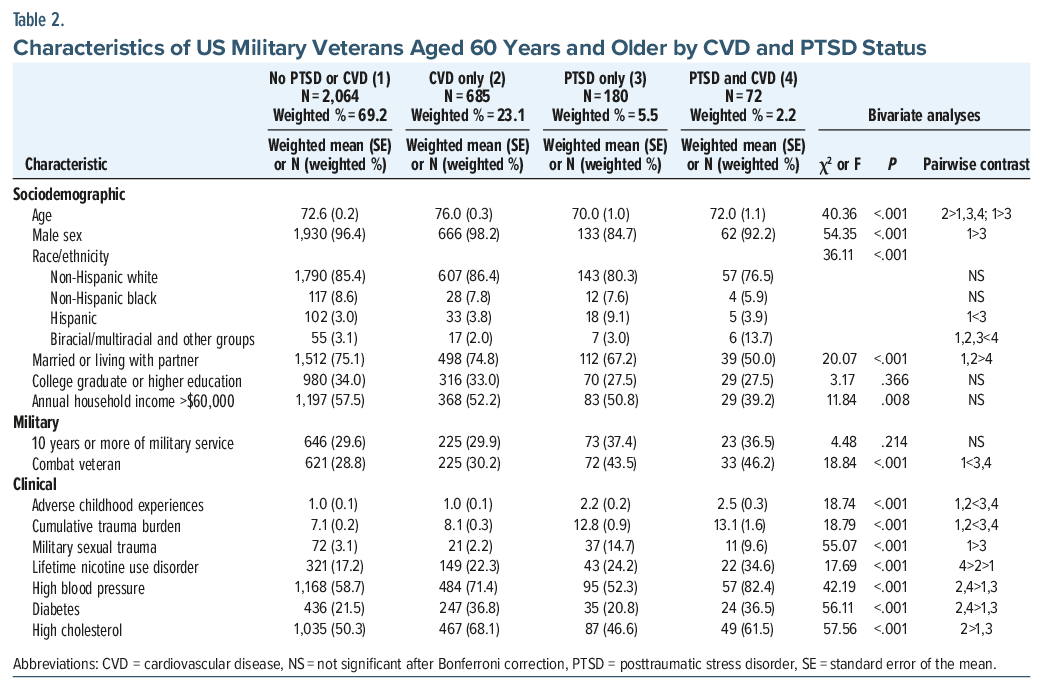
The analytic sample comprised 3,001 US military veterans aged 60 years and older (mean=73.2, SD=7.9, range, 60–99). Most were male (96.1%) and non-Hispanic white (85.2%). As shown in Table 2, a total of 685 veterans (weighted %=23.1%) had CVD only, 180 (weighted % =5.5%) had PTSD only, 72 (weighted % =2.2%) had CVD+PTSD, and 2,064 (weighted % =69.2%) had neither condition.
Correlates of CVD+PTSD
Several factors were significantly associated with CVD+PTSD in multivariable analyses. Compared to controls, veterans with CVD+PTSD were more likely to be combat veterans (OR=1.99, 95% CI, 1.11–3.59) and reported greater exposure to childhood adversity (OR=1.30, 95% CI, 1.15–1.48) and more lifetime traumatic events (OR=1.04, 95% CI, 1.01–1.07). They were also more likely to have a history of nicotine use disorder (OR=1.89, 95% CI, 1.01–3.55) and high blood pressure (OR=2.74, 95% CI, 1.31–5.77) and were less likely to be married or partnered (OR=0.32, 95% CI, 0.18–0.57).
Compared to veterans with CVD only, those with CVD+PTSD were more likely to be combat veterans (OR=2.39, 95% CI, 1.26–4.55) and reported greater exposure to childhood adversity (OR =1.43, 95% CI, 1.23–1.66) and more lifetime traumatic events (OR=1.04, 95% CI, 1.01–1.08). They were also less likely to be married or partnered (OR=0.34, 95% CI, 0.18–0.63). Compared to veterans with PTSD only, those with CVD+PTSD were older (OR =1.05, 95% CI, 1.01–1.11) and more likely to have been diagnosed with high blood pressure (OR= 4.39, 95% CI, 1.96–9.86).
Physical and Mental Health Comorbidities
CVD+PTSD was associated with disproportionately elevated prevalence and odds of a broad range of physical and mental health conditions (Table 3 and Table 4). Compared to controls, veterans with CVD+PTSD had over 13-fold greater odds of major depressive disorder (MDD), 12-fold greater odds of GAD, 9-fold greater odds of cognitive disorder (ie, mild cognitive impairment [MCI], dementia, or Alzheimer disease), nearly 6-fold greater odds of sleep disorder, nearly 5-fold greater odds of reporting concussion or traumatic brain injury (TBI), and higher odds of drug use disorder, chronic pain, kidney disease, arthritis, rheumatoid arthritis, and osteoporosis/osteopenia.
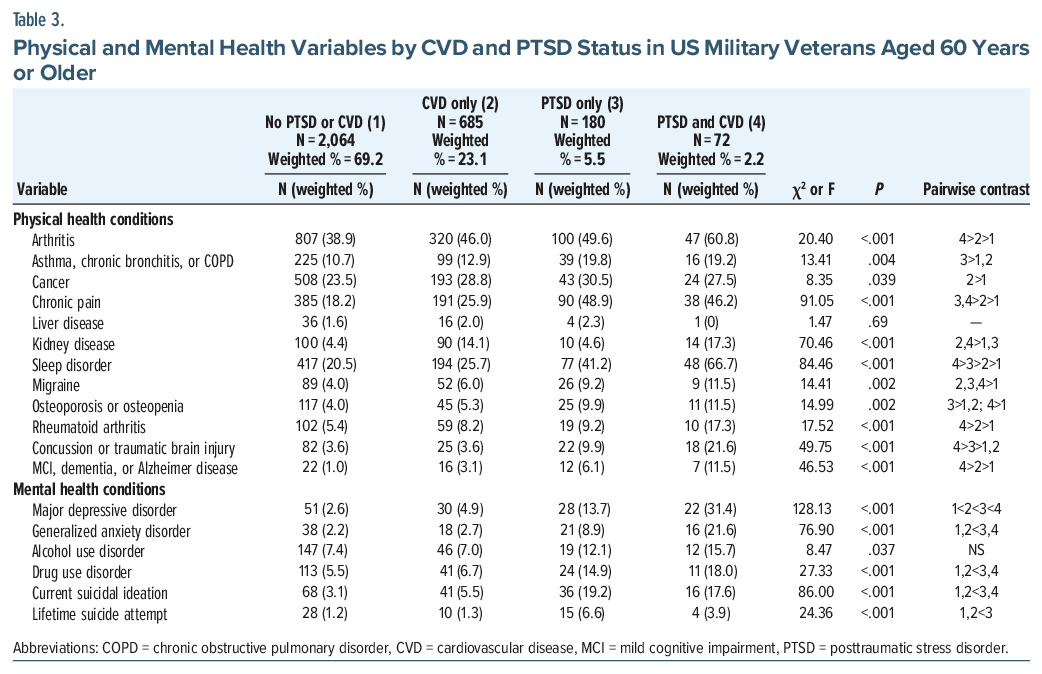
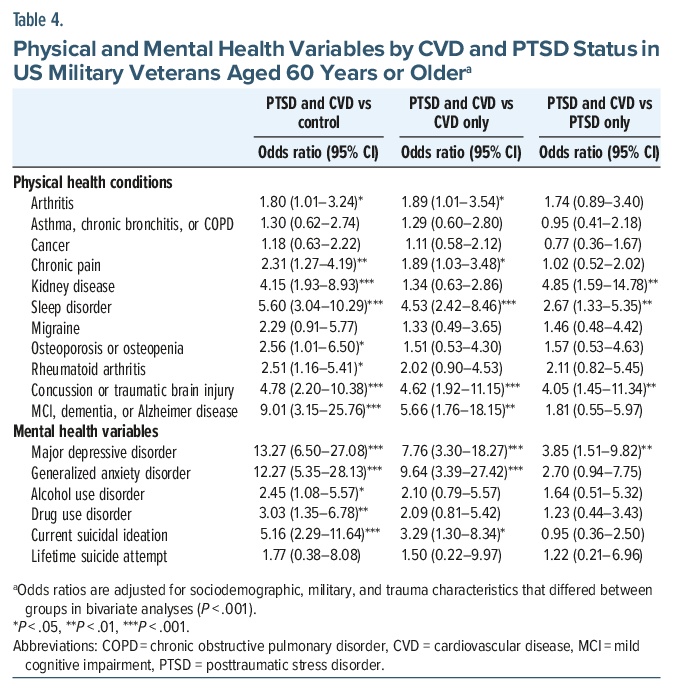
Relative to veterans with CVD only, those with CVD+PTSD had nearly 10-fold greater odds of GAD, nearly 8-fold greater odds of depression, nearly 6-fold greater odds of cognitive disorder, and more than 4.5-fold greater odds of concussion/TBI and sleep disorder, as well as higher odds of current suicidal ideation (SI) and chronic pain. When compared to veterans with PTSD only, those with CVD+PTSD had nearly 5-fold greater odds of kidney disease, 4-fold greater odds of concussion/TBI, nearly 4-fold higher odds of MDD, and more than 2.5-fold greater odds of sleep disorder.
Functioning
In addition to elevated physical and psychiatric health comorbidities, veterans with CVD+PTSD also exhibited the most pronounced functional impairments. As shown in Table 5, compared to those with CVD only, veterans with CVD+PTSD scored lower on measures of overall physical (Cohen d=0.19) and mental (d =0.50) functioning, with moderate magnitude differences observed on measures of cognitive functioning (d =0.66) and psychosocial difficulties (d=0.63); small magnitude differences on measures of mental health (d=0.48), emotional role functioning (d =0.42), social functioning (d =0.35), physical functioning (d= 0.29), absence of bodily pain (d =0.21), and physical role functioning (d =0.20); and minimal differences in vitality (d =0.15) and general health (d=0.12).
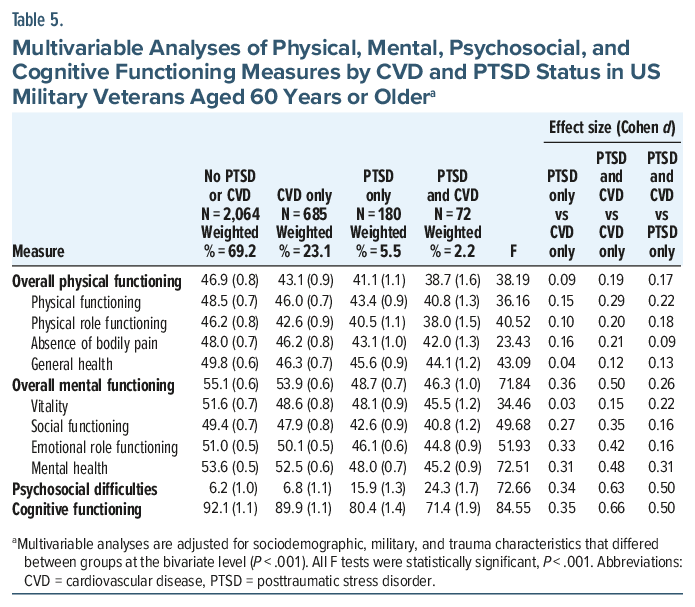
Compared to veterans with PTSD only, veterans with CVD+PTSD also scored lower on measures of overall physical (d= 0.17) and mental (d =0.26) functioning, with moderate magnitude differences in cognitive functioning (d= 0.50) and psychosocial difficulties (d=0.50); small magnitude differences on measures of mental health (d =0.31), vitality (d =0.22), and physical functioning (d= 0.22); and minimal differences in physical role functioning (d=0.18), social functioning (d=0.16), emotional role functioning (d=0.16), general health (d =0.13), and absence of bodily pain (d =0.09).
DISCUSSION
This is the first study, to our knowledge, to characterize the prevalence and health and functional impact of comorbid CVD+PTSD relative to either condition alone in a large, nationally representative sample of older US military veterans. Nearly 1 in 3 (30.8%) US veterans aged 60 years and older were affected by CVD and/or PTSD, which corresponds to an estimated 3.3 million older veterans nationwide.20 Based on observed prevalence rates and national population benchmarks, this includes approximately 2.5 million older veterans with CVD alone, 580,000 with PTSD alone, and 230,000 with both conditions. The high prevalence and substantial physical and mental health burden associated with CVD and PTSD underscore the urgent need for integrated care models that address the complex interplay of these conditions.
In adjusted models, veterans with CVD+PTSD exhibited the poorest outcomes across a range of physical, mental, psychosocial, and cognitive domains compared with single-diagnosis groups. These associations remained significant after adjustment for sociodemographic and military characteristics. The sociodemographic profile of veterans with CVD+PTSD—characterized by lower partnership rates, reduced household income, and greater cumulative trauma exposure—aligns with prior research linking PTSD to increased CVD risk and poorer cardiovascular outcomes.37,38 These sociodemographic and trauma-related vulnerabilities may help explain the elevated psychiatric and cardiovascular burden observed in this subgroup.
Compared with veterans with CVD only, those with CVD+PTSD had nearly 10-fold greater odds of GAD, 8-fold greater odds of MDD, and higher rates of SI and sleep disorder. Alcohol use disorder was elevated only in the comorbid group relative to controls, suggesting that the combination of CVD and PTSD may increase vulnerability to alcohol misuse in older veterans. Moderate reductions in cognitive (d = 0.66) and psychosocial (d = 0.63) functioning were also observed and exceeded those among single diagnosis groups. These findings are consistent with prior evidence linking PTSD to heightened cardiometabolic risk and to behavioral and physiological factors associated with CVD (eg, poor sleep and heightened stress response), which may synergistically worsen symptomatology.39,40
Compared with controls, the co-occurrence of CVD and PTSD conferred more than 12-fold increased odds of MDD and GAD, suggesting additive or interactive effects. Notably, in a large VHA cohort, adjusting for co-occurring psychiatric and behavioral conditions (eg, depression, anxiety, SUD, sleep disorders, and smoking) in addition to physical comorbidities attenuated the association between CVD and PTSD (hazard ratio=0.96, 95% CI, 0.81–1.15) to nonsignificance, suggesting that these factors may mediate the observed link.41 These findings align with prior studies in veteran samples, which document substantial health burdens associated with CVD and PTSD.3 These findings suggest that the link between CVD and PTSD may reflect the accumulation of traumatic stressors and the disproportionate cardiopulmonary disease burden observed in low-income, urban, racial minority populations.42 They further highlight the role of social determinants of health in shaping psychiatric and cardiovascular outcomes and underscore the importance of addressing structural and contextual barriers to care.
PTSD emerged as the strongest correlate of current SI. Veterans with PTSD had approximately 5-fold higher odds of current SI, which was not higher among those with co-occurring CVD. Nevertheless, nearly 1 in 5 veterans with CVD+PTSD reported SI, emphasizing the need for systematic suicide risk screening in both medical and mental health settings that serve trauma-exposed older veterans.
The CVD+PTSD group also demonstrated the most pronounced functional impairments, consistent with meta-analytic data showing neurocognitive deficits in PTSD, particularly in attention/working memory, verbal learning/memory, and processing speed; these impairments appear to be more severe in older adults with PTSD.43,44 In the context of comorbid CVD, these deficits may be exacerbated by cerebrovascular and neurodegenerative processes, potentially explaining the lowest levels of cognitive functioning among veterans with CVD+PTSD. Epidemiologic data further suggest that PTSD is associated with an increased risk of dementia in veterans,45 indicating that CVD+PTSD may represent a particularly high-risk phenotype for late-life cognitive decline.
Several pathophysiological and behavioral mechanisms may contribute to the additive health and functional burden observed in older veterans with comorbid CVD+PTSD: (1) autonomic dysregulation, (2) systemic inflammation, (3) maladaptive health behaviors and sleep disruption, and (4) neurocognitive deficits. Meta-analyses have linked PTSD and anxiety disorders to reduced heart rate variability (HRV), a marker of impaired vagal control.46,47 Large longitudinal studies, such as Framingham and the Atherosclerosis Risk in Communities study, found that reduced HRV is associated with an elevated risk for cardiovascular events in individuals without CVD.48,49 HRV impairment may be further exacerbated by sleep apnea, a highly prevalent condition in both PTSD and CVD, which independently increases cardiovascular risk.50 PTSD is also associated with systemic inflammation, as reflected by elevated markers such as C-reactive protein and intercellular adhesion molecule-1 and endothelial dysfunction, which contribute to atherosclerosis. These effects may be amplified by depression, pain, and SUD.51,52 Maladaptive health behaviors and disrupted sleep may also link PTSD with adverse cardiovascular outcomes. Depression, anxiety, and SUD, which were most prevalent in older veterans with CVD+PTSD, are associated with smoking, physical inactivity, and fragmented sleep, which can increase cardiometabolic risk.40,53,54 Finally, PTSD is associated with neurocognitive deficits in attention, processing speed, and memory,44 which may impair self-management of complex cardiovascular care regimens, thus compounding vulnerability to adverse health and functional outcomes.
Collectively, these findings underscore the importance of integrated cardiovascular and mental health care for older veterans. Routine bidirectional screening for both cardiovascular and mental health conditions may be warranted, given the heightened health and functional burden observed in the CVD+PTSD group. The American Heart Association has emphasized the importance of the mind-heart-body connection and recommends the integration of psychological assessment and treatment into CVD prevention efforts.54 Trauma-focused psychotherapies and integrated behavioral health interventions may also enhance functional outcomes in this population.55 For example, meta-analytic evidence has revealed moderate functional gains following PTSD psychotherapy,56 and intensive cognitive processing therapy has demonstrated sustained improvements in physical, mental, and social functioning among veterans,13 with effects persisting for up to 12 months.57 Although the impact of trauma-focused treatments on cardiovascular endpoints remains to be elucidated, treating PTSD and co-occurring conditions may help improve modifiable risk factors, such as poor sleep, that contribute to cardiometabolic risk.58
This study has several limitations. First, its cross-sectional design precludes causal inference, and reverse causation (eg, CVD precipitating PTSD symptoms) cannot be ruled out. Second, CVD was assessed via self-report of a physical or other health care professional diagnosis, which may underestimate undiagnosed disease. Third, PTSD and other mental health and functioning measures were assessed using self-report measures rather than diagnostic interviews. Fourth, consistent with the demographic composition of US veterans, the sample was predominantly male and white, which may limit generalizability to more diverse veteran populations. Fifth, unmeasured factors such as sleep apnea, pain severity, medication effects, and social determinants of health may also have influenced the observed associations.
CONCLUSIONS
Older veterans with comorbid CVD+PTSD represent a high-need clinical subgroup characterized by concentrated physical and mental health comorbidities, as well as marked psychosocial and cognitive impairments. These findings highlight the importance of trauma-informed, integrated models of care that address both cardiovascular and mental health needs. Early detection and management of modifiable risk factors, such as smoking, inactivity, poor sleep, and co-occurring depression, anxiety, and substance use, may help reduce downstream cardiovascular risk. Evidence-based PTSD treatments may also help improve health behaviors and functioning, with the potential to improve long-term outcomes. Future research should examine whether PTSD treatment reduces cardiometabolic risk, incorporate physiological measures to elucidate mechanisms, and evaluate the efficacy of integrated interventions on both CVD- and PTSD-relevant outcomes. Longitudinal studies are also needed to evaluate long-term risk for cognitive decline and dementia in this vulnerable segment of the veteran population.
Article Information
Published Online: July 14, 2026. https://doi.org/10.4088/PCC.26m04187
© 2026 Physicians Postgraduate Press, Inc.
Submitted: January 14, 2026; accepted March 20, 2026.
To Cite: Yang A, Manaswi A, Fischer MW, et al. Comorbid cardiovascular disease and posttraumatic stress disorder in older US veterans: prevalence, health burden, and functional impairment. Prim Care Companion CNS Disord 2026;28(4):26m04187.
Author Affiliations: Scarsdale High School, Scarsdale, New York (Yang); Yale University, New Haven, Connecticut (Manaswi); VA Connecticut Healthcare System, West Haven, Connecticut (Fischer, Na); US Department of Veterans Affairs National Center for PTSD, VA Connecticut Healthcare System, West Haven, Connecticut (Fischer, Pietrzak); Department of Psychiatry, Yale School of Medicine, New Haven, Connecticut (Fischer, Na, Pietrzak); Department of Social and Behavioral Sciences, Yale School of Public Health, New Haven, Connecticut (Pietrzak).
Corresponding Author: Robert H. Pietrzak, PhD, MPH, National Center for PTSD, VA Connecticut Healthcare System, 950 Campbell Ave, West Haven, CT 06516 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Acknowledgments: The authors thank the veterans who participated in the National Health and Resilience in Veterans Study.
Clinical Points
- Older veterans with comorbid CVD+PTSD have a markedly elevated burden of health and functional difficulties, underscoring the importance of integrated, trauma-informed care to improve outcomes in this high-risk population.
- Early detection and management of modifiable risk factors, such as smoking, inactivity, poor sleep, and co-occurring depression, anxiety, and substance use, may help reduce downstream cardiovascular risk.
References (58)

- Yazdanyar A, Newman AB. The burden of cardiovascular disease in the elderly: morbidity, mortality, and costs. Clin Geriatr Med. 2009;25(4):563–vii.
- Zhou M, Zhao G, Zeng Y, et al. Aging and cardiovascular disease: current status and challenges. Rev Cardiovasc Med. 2022;23(4):135.
- Arechiga CG, Yang R, Pietrzak RH. Prevalence, correlates, and mental and physical health burden of cardiovascular disease in older U.S. military veterans. PLoS Ment Health. 2024;1(7):e0000192. CrossRef
- Assari S. Veterans and risk of heart disease in the United States: a cohort with 20 years of follow up. Int J Prev Med. 2014;5(6):703–709. PubMed
- Hinojosa R. Cardiovascular disease among United States military veterans: evidence of a waning healthy soldier effect using the National Health Interview Survey. Chronic Illn. 2018;16(1):55–68. CrossRef
- Olson DE, Zhu M, Long Q, et al. Increased cardiovascular disease, resource use, and costs before the clinical diagnosis of diabetes in veterans in the southeastern U.S. J Gen Intern Med. 2015;30(6):749–757. PubMed CrossRef
- Vance MC, Wiitala WL, Sussman JB, et al. Increased cardiovascular disease risk in veterans with mental illness. Circ Cardiovasc Qual Outcomes. 2019;12(10):e005563.
- Betancourt JA, Granados PS, Pacheco GJ, et al. Exploring health outcomes for U.S. veterans compared to non-veterans from 2003 to 2019. Healthcare. 2021;9(5):604. CrossRef
- Zuo W, Wu J. The interaction and pathogenesis between cognitive impairment and common cardiovascular diseases in the elderly. Ther Adv Chronic Dis. 2022;13:20406223211063020. CrossRef
- Wisco BE, Nomamiukor FO, Marx BP, et al. Posttraumatic stress disorder in US military veterans: results from the 2019-2020 national health and Resilience in veterans study. J Clin Psychiatry. 2022;83(2):20m14029.
- Gros DF, Szafranski DD, Brady KT, et al. Relations between pain, PTSD symptoms, and substance use in veterans. Psychiatry. 2015;78(3):277–287. CrossRef
- Shor R, Borowski S, Zelkowitz RL, et al. The transition to civilian life: impact of comorbid PTSD, chronic pain, and sleep disturbance on veterans’ social functioning and suicidal ideation. Psychol Trauma. 2023;15(8):1315–1323. CrossRef
- Smith DL, Kovacevic M, Montes M, et al. Improving mental, physical, and social functioning through participation in a 3-week cognitive processing therapy-based intensive PTSD treatment. J Anxiety Disord. 2022;88:102560. CrossRef
- Schnurr PP, Lunney CA. Work-related outcomes among female veterans and service members after treatment of posttraumatic stress disorder. Psychiatr Serv. 2012;63(11):1072–1079. PubMed CrossRef
- Miller CR, McDonald JE, Grau PP, et al. Quality of life in posttraumatic stress disorder: the role of posttraumatic anhedonia and depressive symptoms in a treatment-seeking community sample. Trauma Care. 2024;4(1):87–97. CrossRef
- Seligowski AV, Ressler KJ. Sex differences in the co-occurrence of PTSD and cardiovascular disease. Psychiatr Ann. 2022;52(1):26–30. CrossRef
- Khan N, Iqra Tanveer Khan S, Joti S, et al. Association of cardiovascular diseases with post-traumatic stress disorder: an updated review. Cardiol Rev. 2025;33(5):441–447.
- Stellman SD, Pless Kaiser A, Smith BN, et al. Impact of persistent combat-related PTSD on heart disease and chronic disease comorbidity in aging Vietnam veterans. J Occup Environ Med. 2025;67(5):299–305. CrossRef
- Reinke LF, Vig EK, Tartaglione EV, et al. Symptom burden and palliative care needs among high-risk veterans with multimorbidity. J Pain Symptom Manag. 2019;57(5):880–889. CrossRef
- U.S. Census Bureau. Current Population Survey, August 2019: Veterans Supplement – Technical Documentation. U.S. Department of Commerce; 2019. https://www2.census.gov/programs-surveys/cps/techdocs/cpsaug19.pdf
- Pietrzak RH, Goldstein RB, Southwick SM, et al. Medical comorbidity of full and partial posttraumatic stress disorder in US adults: results from Wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. Psychosom Med. 2011;73(8):697–707. PubMed CrossRef
- Weathers FW, Litz BT, Keane TM, et al. The PTSD Checklist for DSM-5 (PCL-5). Scale available from the National Center for PTSD at. www.ptsd.va.gov
- Weathers FW, Blake DD, Schnurr PP, et al. The Life Events Checklist for DSM-5 (LEC-5). 2013. Instrument available from the National Center for PTSD at. www.ptsd.va.gov
- Bovin MJ, Marx BP, Weathers FW, et al. Psychometric properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (PCL-5) in veterans. Psychologic Assess. 2016;28(11):1379–1391. PubMed CrossRef
- Kroenke K, Spitzer RL, Williams JBW. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. PubMed CrossRef
- Kroenke K, Spitzer RL, Williams JBW, et al. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146(5):317–325. PubMed CrossRef
- Babor TF, Higgins-Biddle JC, Saunders JB, et al. The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care. World Health Organization; 2001.
- Tiet QQ, Leyva YE, Moos RH, et al. Screen of Drug Use: diagnostic accuracy of a new brief tool for primary care. JAMA Intern Med. 2015;175(8):1371–1377. PubMed CrossRef
- Heatherton TF, Kozlowski LT, Frecker RC, et al. The Fagerstrom test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. Addiction. 1991;86(9):1119–1127.
- Osman A, Bagge CL, Gutierrez PM, et al. The Suicide Behaviors Questionnaire-Revised (SBQ-R): validation with clinical and nonclinical samples. Assessment. 2001;8(4):443–454.
- Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am J Prev Med. 1998;14(4):245–258. PubMed CrossRef
- Stewart AL, Ware JE. Measuring Functioning and Well Being: The Medical Outcomes Study Approach. Duke University Press; 1992. CrossRef
- Marx BP, Schnurr PP, Lunney C, et al. The Brief Inventory of Psychosocial Functioning (B-IPF); 2019.
- Stewart AL, Ware JE Jr, Sherbourne CD, et al. Psychological distress/well-being and cognitive functioning measures. In: Stewart ALW JE, ed. Measuring Functioning and Well-Being: The Medical Outcomes Study Approach. Duke University Press;1992:102–142.
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. Routledge; 1988. CrossRef
- Wilson DB. Practical Meta-Analysis Effect Size Calculator. Accessed August 23, 2025. https://www.campbellcollaboration.org/research-resources/effect-size-calculator-html
- Edmondson D, von Känel R. Post-traumatic stress disorder and cardiovascular disease. Lancet Psychiatry. 2017;4(4):320–329.
- Kubzansky LD, Koenen KC, Spiro A 3rd, et al. Prospective study of posttraumatic stress disorder symptoms and coronary heart disease in the Normative Aging Study. Arch Gen Psychiatry. 2007;64(1):109–116. PubMed CrossRef
- O’Donnell CJ, Schwartz Longacre L, Cohen BE, et al. Posttraumatic stress disorder and cardiovascular disease: state of the science, knowledge gaps, and research opportunities. JAMA Cardiol. 2021;6(10):1207–1216.
- Meinhausen C, Prather AA, Sumner JA. Posttraumatic stress disorder (PTSD), sleep, and cardiovascular disease risk: a mechanism-focused narrative review. Health Psychol. 2022;41(10):663–673. CrossRef
- Scherrer JF, Salas J, Cohen BE, et al. Comorbid conditions explain the association between posttraumatic stress disorder and incident cardiovascular disease. JAHA. 2019;8(4):e011133. CrossRef
- Taylor-Clift A, Holmgreen L, Hobfoll SE, et al. Traumatic stress and cardiopulmonary disease burden among low-income, urban heart failure patients. J Affect Disord. 2016;190:227–234. PubMed CrossRef
- Schuitevoerder S, Rosen JW, Twamley EW, et al. A meta-analysis of cognitive functioning in older adults with PTSD. J Anxiety Disord. 2013;27(6):550–558.
- Scott JC, Matt GE, Wrocklage KM, et al. A quantitative meta-analysis of neurocognitive functioning in posttraumatic stress disorder. Psychol Bull. 2015;141(1):105–140.
- Yaffe K, Vittinghoff E, Lindquist K, et al. Posttraumatic stress disorder and risk of dementia among US veterans. Arch Gen Psychiatry. 2010;67(6):608–613. PubMed CrossRef
- Chalmers JA, Quintana DS, Abbott MJA, et al. Anxiety disorders are associated with reduced heart rate variability: a meta-analysis. Front Psychiatry. 2014;5:80.
- Schneider M, Schwerdtfeger A. Autonomic dysfunction in posttraumatic stress disorder indexed by heart rate variability: a meta-analysis. Psychol Med. 2020;50(12):1937–1948. PubMed CrossRef
- Tsuji H, Larson MG, Venditti FJ Jr, et al. Impact of reduced heart rate variability on risk for cardiac events. The Framingham Heart Study. Circulation. 1996;94(11):2850–2855. PubMed CrossRef
- Liao D, Cai J, Rosamond WD, et al. Cardiac autonomic function and incident coronary heart disease: a population-based case-cohort study. The ARIC Study. Atherosclerosis Risk in Communities Study. Am J Epidemiol. 1997;145(8):696–706. PubMed CrossRef
- Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease. Circulation. 2008;118(10):1080–1111.
- Passos IC, Vasconcelos-Moreno MP, Costa LG, et al. Inflammatory markers in post-traumatic stress disorder: a systematic review, meta-analysis, and meta-regression. Lancet Psychiatry. 2015;2(11):1002–1012. PubMed CrossRef
- Plantinga L, Bremner JD, Miller AH, et al. Association between posttraumatic stress disorder and inflammation: a twin study. Brain Behav Immun. 2013;30:125–132. PubMed CrossRef
- Saguin E, Gomez-Merino D, Sauvet F, et al. Sleep and PTSD in the military forces: a reciprocal relationship and a psychiatric approach. Brain Sci. 2021;11(10):1310. CrossRef
- Levine GN, Cohen BE, Commodore-Mensah Y, et al. Psychological health, well-being, and the mind-heart-body connection: a scientific statement from the American Heart Association. Circulation. 2022;143(10):e763–e783.
- Lely JCG, Kleber RJ. From pathology to intervention and beyond. Reviewing current evidence for treating trauma-related disorders in later life. Front Psychiatry. 2022;13:814130. CrossRef
- Bonfils KA, Tennity CL, Congedo BA, et al. Functional outcomes from psychotherapy for people with posttraumatic stress disorder: a meta-analysis. J Anxiety Disord. 2022;89:102576. CrossRef
- Held P, Smith LJ, Parmar AM, et al. Veterans’ 12-month PTSD and depression outcomes following 2- and 3-week intensive cognitive processing therapy-based treatment. Eur J Psychotraumatol. 2024;15(1):2350908. CrossRef
- Miller KE, Brownlow JA, Gehrman PR. Sleep in PTSD: treatment approaches and outcomes. Curr Opin Psychol. 2020;34:12–17.
Please sign in or purchase this PDF for $40.