Fluoxetine is generally a well-tolerated selective serotonin reuptake inhibitor (SSRI), but can rarely cause significant adverse effects, including hepatotoxicity. While asymptomatic liver enzyme elevations occur in 0.5%–1% of cases, severe and life-threatening drug-induced liver injury (DILI) is exceedingly rare.1,2 We report a case of fluoxetine-induced acute liver injury in a young woman to highlight the possibility of severe hepatic damage with a widely used antidepressant and to emphasize the importance of vigilant monitoring, even at standard doses, especially in primary care.
Case Report
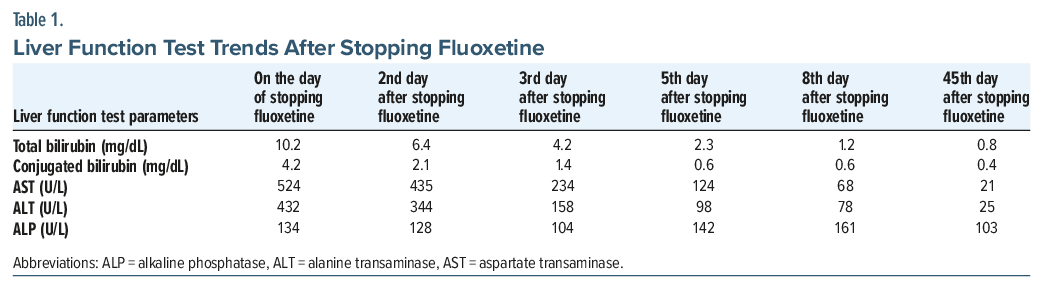
A 29-year-old woman presented in October 2023 with a 6-month history of suspiciousness, social withdrawal, self-absorbed behavior, and unprovoked aggression. She was diagnosed with schizophrenia (ICD-10: F20.0) and initiated on aripiprazole 5 mg, titrated to 10 mg. After 1 month, she demonstrated approximately 40% improvement on the Positive and Negative Syndrome Scale3 but developed marked akathisia. Aripiprazole was cross-tapered to risperidone 3 mg. However, extrapyramidal symptoms necessitated dose reduction to 2 mg. Over the next 2 months, she achieved 80%–90% improvement. Despite remission of psychotic symptoms, she gradually developed pervasive low mood, anhedonia, depressive cognitions, and suicidal ideation. She was admitted to the hospital in January 2024 and diagnosed with post-schizophrenic depression (ICD-10: F20.4). On the Calgary Depression Scale for Schizophrenia,4 she scored 20, indicating severe depression. Baseline investigations, including liver function tests (LFTs), were within normal limits. Fluoxetine 20 mg was initiated alongside risperidone and titrated to 40 mg over 2 weeks, resulting in significant improvement in depressive symptoms. She was discharged in stable condition and remained well during the following 2 months taking fluoxetine 40 mg and risperidone 2 mg, with complete resolution of symptoms and functional recovery. Gradually, her mother noted yellowing of the eyes, reduced appetite, and marked weakness, prompting re-evaluation. Examination revealed pallor and icterus. Laboratory investigations demonstrated significantly elevated bilirubin and liver enzymes (Table 1), along with iron-deficiency anemia, which led to readmission in March 2024. Comprehensive evaluation excluded alternative etiologies, including viral and autoimmune hepatitis. The treatment team considered the possibility of DILI and discontinued fluoxetine. Risperidone was continued with close monitoring, with plans to taper if LFTs remained elevated. Iron supplementation was initiated. LFT levels normalized within 6 to 7 days of fluoxetine withdrawal (Table 1). The Naranjo Adverse Drug Reaction Probability Scale5 score was 6, indicating a probable drug-related adverse event. Following fluoxetine discontinuation, the patient again developed severe depressive symptoms with suicidal ideation. After normalization of liver function, escitalopram was initiated at 5 mg and titrated to 20 mg over 2 weeks. Given presence of persistent suicidal ideation, oral ketamine was administered on alternate days, leading to significant clinical improvement. Serial LFT monitoring during hospitalization and at 6-week and 3-month follow-up remained within normal limits (Table 1). She continues to remain stable on the current regimen, with plans for regular monitoring of liver function and other side effects.
Discussion
In this case, the patient presented with a ≥5 times elevation in liver enzymes, a rare but clinically significant manifestation of DILI that can be life-threatening if not promptly managed.6 Among antidepressants, SSRIs are generally considered to have a lower risk of hepatotoxicity compared to other classes. Among SSRIs, escitalopram and citalopram are preferred in patients with underlying liver impairment due to their more favorable hepatic profile.7 In contrast, fluoxetine, with its long half-life and active metabolites extensively metabolized via hepatic pathways, is relatively less preferred. There are 3 published reports describing clinically significant and life-threatening hepatitis due to fluoxetine, all in patients with depression, whereas our case is unique in that it occurred in the context of schizophrenia.8–10 Rapid normalization of liver enzymes after drug cessation was also notable.
The mechanisms behind this adverse effect are not well understood but are hypothesized to include direct hepatotoxicity, mitochondrial damage, and cholestatic injury.6 The patient’s sensitivity to multiple medications at lower doses suggests she may be a poor metabolizer, which could have contributed to the DILI.11–13
Article Information
Published Online: June 30, 2026. https://doi.org/10.4088/PCC.26cr04182
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(4):26cr04182
Submitted: January 7, 2026; accepted March 18, 2026.
To Cite: Tekupalli ST, Bakam A, Mamidipalli SS, et al. Fluoxetine-induced liver injury in a patient with post-schizophrenic depression. Prim Care Companion CNS Disord 2026;28(4):26cr04182.
Author Affiliations: Department of Psychiatry, All India Institute of Medical Sciences, Bibinagar, Hyderabad, India (all authors).
Corresponding Author: Anirudh Bakam, MD, All India Institute of Medical Sciences, Bibinagar, Hyderabad-508126, Telangana, India ([email protected])
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient and family members to publish the case report, and information has been de-identified, including dates, to protect patient anonymity.
ORCID: Shushsnk Tej Tekupalli: https://orcid.org/0009-0009-7738-3082
References (13)

- Carvajal García-Pando A, García del Pozo J, Sánchez AS, et al. Hepatotoxicity associated with the new antidepressants. J Clin Psychiatry. 2002;63(2):135–137. PubMed CrossRef
- Devarbhavi H, Raj S, Aradya VH, et al. Drug-induced liver injury associated with Stevens-Johnson syndrome/toxic epidermal necrolysis: patient characteristics, causes, and outcome in 36 cases. Hepatology. 2016;63(3):993–999. PubMed CrossRef
- Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. PubMed CrossRef
- Addington D, Addington J, Maticka-tyndale E. Assessing depression in schizophrenia: the Calgary Depression Scale. Br J Psychiatry. 1993;163(S22):39–44. PubMed
- Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. PubMed CrossRef
- Aithal GP, Watkins PB, Andrade RJ, et al. Case definition and phenotype standardization in drug-induced liver injury. Clin Pharmacol Ther. 2011;89(6):806–815. PubMed CrossRef
- Taylor DM, Barnes TRE, Young AH. The Maudsley Prescribing Guidelines in Psychiatry, 14th Edition. 14th ed. John Wiley & Sons; 2021.
- Cai Q, Benson MA, Talbot TJ, et al. Acute hepatitis due to fluoxetine therapy. Mayo Clin Proc. 1999;74(7):692–694. PubMed CrossRef
- Lyssy LA, Mui R, Griffin M. S3291 A unique case of drug induced liver injury related to fluoxetine. Official J Am Coll Gastroenterology (ACG). 2022;117(10S):e2093. CrossRef
- Soni A, Mane A. Fluoxetine-induced liver injury and skin reaction: a case report. Indian J Psychiatry. 2021;63(4):405–406. PubMed CrossRef
- Miners JO, Birkett DJ. Cytochrome P4502C9: an enzyme of major importance in human drug metabolism. Br J Clin Pharmacol. 1998;45(6):525–538. PubMed CrossRef
- Pirmohamed M, Park B. Cytochrome P450 enzyme polymorphisms and adverse drug reactions. Toxicology. 2003;192(1):23–32. PubMed CrossRef
- Wilkinson GR. Genetic variability in cytochrome P450 3A5 and in vivo cytochrome P450 3A activity: some answers but still questions. Clin Pharmacol Ther. 2004;76(2):99–103. PubMed CrossRef
Please sign in or purchase this PDF for $40.