Abstract
Objective: To review conclusive evidence concerning the usage, efficacy, and side effects of 2 N-methyl-D-aspartate (NMDA) receptor antagonists, memantine and amantadine, in children with autism spectrum disorder (ASD) to determine their effectiveness in treating associated core and comorbid conditions.
Data Sources: A comprehensive literature search was conducted across multiple electronic databases, utilizing a combination of controlled vocabulary and keywords: autism spectrum disorder, autistic disorder, Asperger’s, PDD-NOS, neurodevelopmental disorders, memantine, amantadine, and NMDA receptor antagonist.
Study Selection: The initial screening identified 87 studies, and 11 were selected for full review. A total of 8 studies met the inclusion criteria of the qualitative synthesis and were included in the systematic review. The inclusion criteria were children aged <18 years with an ASD diagnosis, studies assessing amantadine or memantine with a comparison of placebo or treatment as usual, studies reporting clinical improvement in common ASD symptoms, and clinical trials or retrospective chart reviews. Exclusion criteria included unpublished data and multiple reports from the same dataset.
Data Extraction: Data were extracted using a standardized form focused on study design and validity domains. Multiple reviewers independently abstracted data, with discrepancies resolved by consensus.
Data Synthesis: Memantine and amantadine demonstrated favorable safety profiles. However, the evidence regarding their efficacy in addressing core ASD symptoms was inconclusive. Memantine was associated with potential improvements in cognitive and behavioral outcomes, though the evidence was confounded by methodological limitations. Amantadine showed potential in adjunctive treatment with risperidone, particularly in mitigating disruptive behaviors, but variability in outcomes between parent-reported and clinician-assessed measures raised concerns about the reliability and robustness of the findings.
Conclusions: This systematic review highlights the need for large-scale, multicenter, double-blind, randomized controlled trials with rigorously standardized assessment tools and diverse clinical populations to better define the therapeutic potential and establish guidelines for the use of memantine and amantadine in ASD.
Prim Care Companion CNS Disord 2026;28(4):25r04152
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Autism spectrum disorder (ASD) is a complex neurodevelopmental condition characterized by persistent deficits in social communication and interpersonal skills, alongside restricted, repetitive patterns of behavior, interests, or activities. In the United States, it is estimated that 1 in 36 children is on the autism spectrum.1 Despite its prevalence, ASD remains difficult to diagnose due to heterogeneous presentations and the lack of biomarkers.1 The presence of comorbid conditions further complicates diagnosis and treatment, with up to 70% of individuals with ASD experiencing neuropsychiatric comorbidities such as intellectual disabilities, attention-deficit/hyperactivity disorder (ADHD), anxiety, depression, sleep disturbances, epilepsy, and gastrointestinal issues.2 These overlapping symptoms can lead to diagnostic overshadowing. Current treatments primarily involve behavioral and educational interventions, speech therapy, and medications to manage comorbid symptoms. However, there remains a significant gap in evidence-based pharmacologic treatments targeting the core symptoms of ASD, such as deficits in social communication and repetitive behaviors. Currently, only 2 US Food and Drug Administration–approved medications, risperidone and aripiprazole, are available to treat irritability associated with ASD,3,4 highlighting the need for further exploration of psychopharmacologic interventions.
Recent research has focused on investigating the glutamate hypothesis. The glutamate hypothesis in ASD suggests that disruptions in the balance between excitatory and inhibitory neurotransmission, particularly involving glutamate (Glu) and γ-aminobutyric acid (GABA), play a key role in the neurophysiology of ASD.5,6 Synaptic plasticity, essential for neurodevelopment and cognitive functioning, may be altered in ASD due to this excitatory-inhibitory imbalance.6 Research shows that altered glutamatergic and GABAergic systems affect functional brain connectivity, which could underlie clinical symptoms such as deficits in social communication and repetitive behaviors.5,6 In particular, changes in glutamate concentrations in regions like the anterior cingulate cortex have been linked to functional dysconnectivity and more severe communication impairments in individuals with ASD.7 This evidence supports the theory that glutamatergic dysregulation contributes to the pathophysiology of ASD, potentially disrupting large-scale brain networks during resting-state functional magnetic resonance imaging studies.6
N-methyl-D-aspartate (NMDA) receptors, a type of glutamate receptor, have been implicated in learning, memory, and synaptic plasticity.6 Preliminary reports have sparked interest in NMDA receptor antagonists, such as memantine and amantadine, as potential interventions for core ASD symptoms.8–11 However, initial trials have shown mixed results, indicating a need for comprehensive, high-quality studies to determine the therapeutic effectiveness of NMDA receptor antagonists among individuals with ASD, either for core symptoms of ASD or for management of comorbidities. We conducted a thorough review of all available data, including reports of clinical application, concerning the usage, efficacy, and side effects of 2 NMDA receptor antagonists, memantine and amantadine, in children with ASD to determine conclusive evidence for their effectiveness in treating both core and comorbid conditions associated with ASD.
METHODS
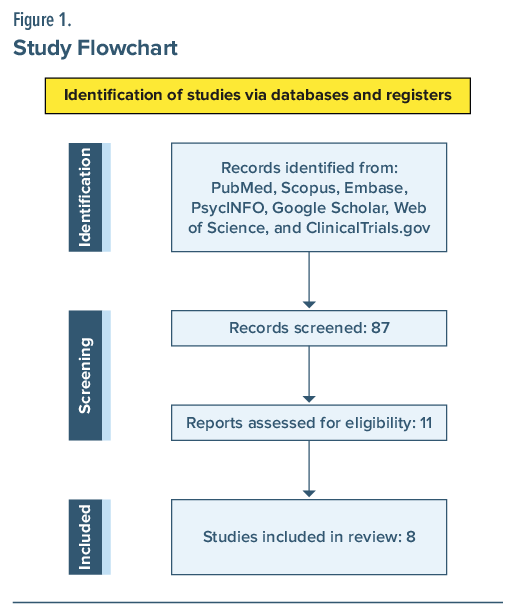
The systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Figure 1). A comprehensive search was conducted across several databases from their inception to November 24, 2023. These databases included PubMed, Scopus, Embase, PsycINFO, Google Scholar, and Web of Science. Databases of ongoing clinical trials were also searched via www.clinicaltrials. gov.
Study Design and Eligibility Criteria
Coauthors N.G. and M.G. designed the search strategy, utilizing a combination of controlled vocabulary and keywords: autism spectrum disorder, autistic disorder, Asperger’s, PDD-NOS, neurodevelopmental disorders, memantine, amantadine, and NMDA receptor antagonist. The search was not restricted by language but was limited to studies involving human subjects. To further reduce selection bias, references from included studies were manually reviewed.
Selection and Eligibility Process
Two independent reviewers (N.G. and M.G.) screened the titles and abstracts of potentially relevant articles. After the initial screening, full-text articles of eligible studies were separately reviewed. The systematic search focused on studies involving individuals aged <18 years diagnosed with ASD per Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), DSM-IV-TR, or DSM-III criteria. The inclusion criteria, using the PICOS framework (Population, Intervention, Comparison, Outcome, Study Design), were as follows:
- P: Children aged <18 years with an ASD diagnosis
- I: Studies assessing amantadine or memantine
- C: Placebo or treatment as usual
- O: Studies reporting clinical improvement in common ASD symptoms, such as core symptoms, ADHD, depression, anxiety, mood instability/irritability, and cognitive symptoms
- S: Clinical trials or retrospective chart reviews.
Exclusion criteria included unpublished data and multiple reports from the same dataset (only original studies were considered to avoid duplication). For missing data, the corresponding authors of the articles were contacted. The 2 reviewers used a standardized data extraction form to collect data from the selected studies.
RESULTS
The comprehensive search identified 87 articles, of which 11 studies were selected for eligibility. A total of 8 studies met the inclusion criteria and were included in the systematic review. These included 3 randomized controlled trials (RCTs) on memantine,13,14,16 1 review of 3 clinical trials on memantine,15 2 RCTs on amantadine,8,10 1 open-label trial on memantine,12 and 1 retrospective study on amantadine.11 Five of the 8 studies were conducted in the United States, 2 were studies conducted in Iran, and the final one was a multicenter study. A detailed examination of the studies, including their methodologies, findings, and limitations, is provided in the subsequent sections and in Table 1.
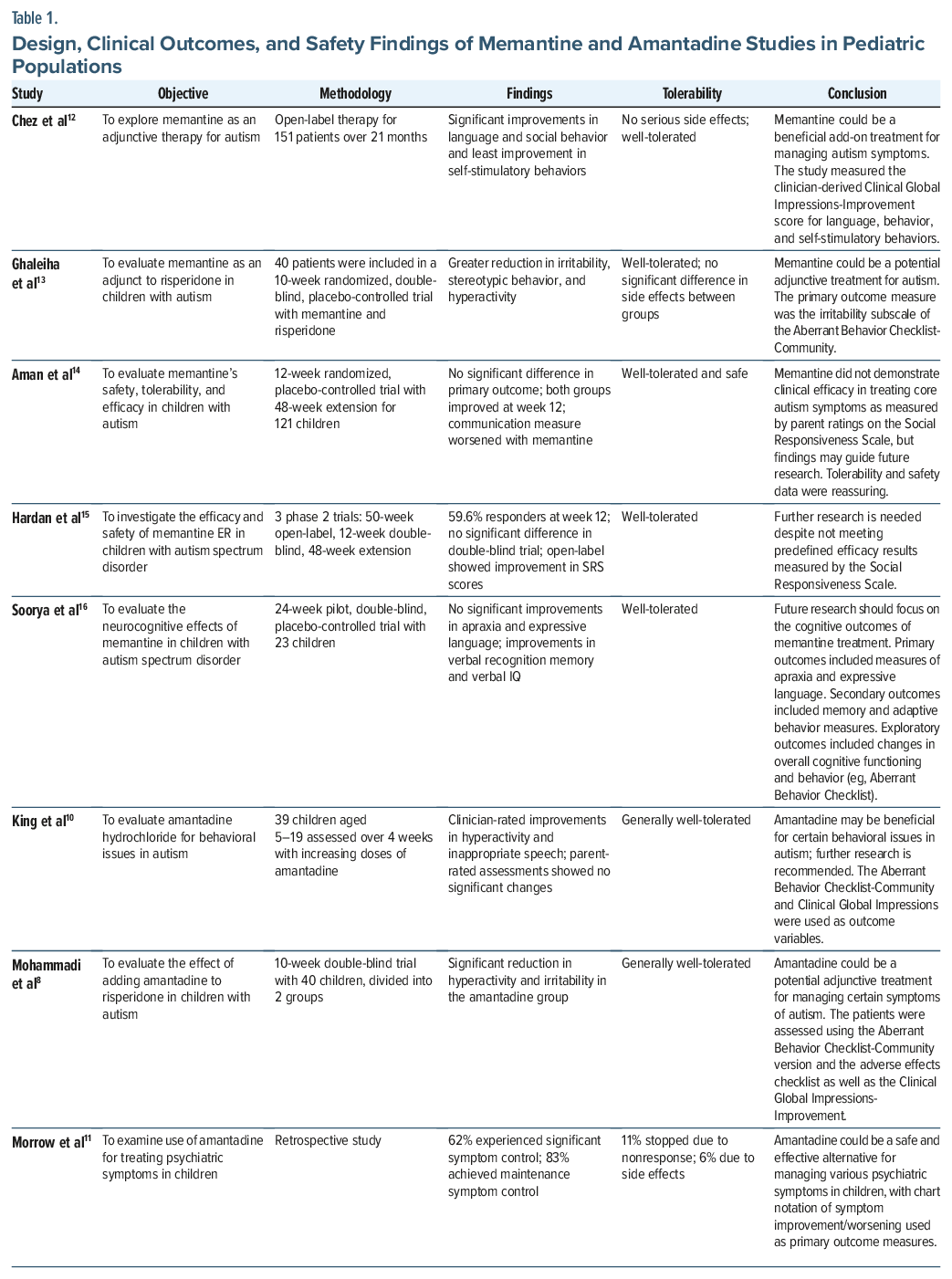
Memantine showed promise in initial trials,12,13 but these positive findings were not reproduced in subsequent trials.14 In a small-scale study, an improvement in verbal recognition memory, as assessed by the Narrative Memory-Recognition test, was observed following the use of memantine.16 Similarly, initial clinical trials with amantadine showed promise both as a monotherapy10 and in combination with risperidone.8 According to a study, 40 of 59 candidates with ASD experienced positive effects with ADHD symptoms after taking amantadine for 3 months or longer.11
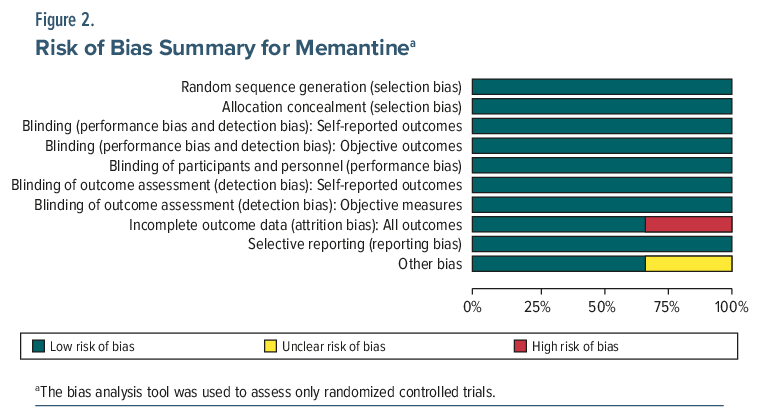
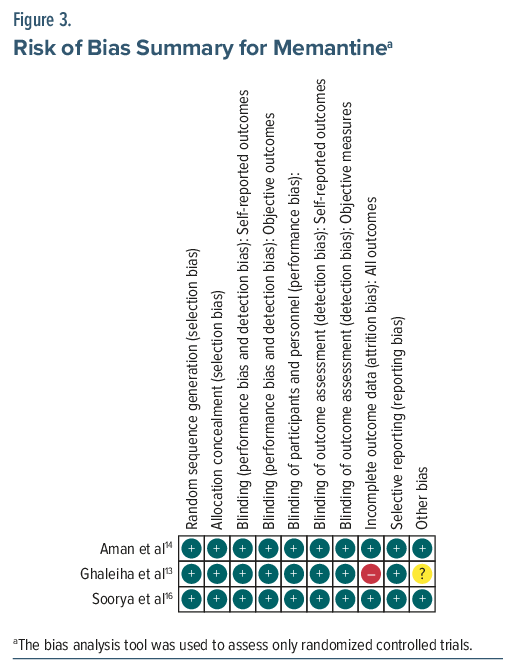
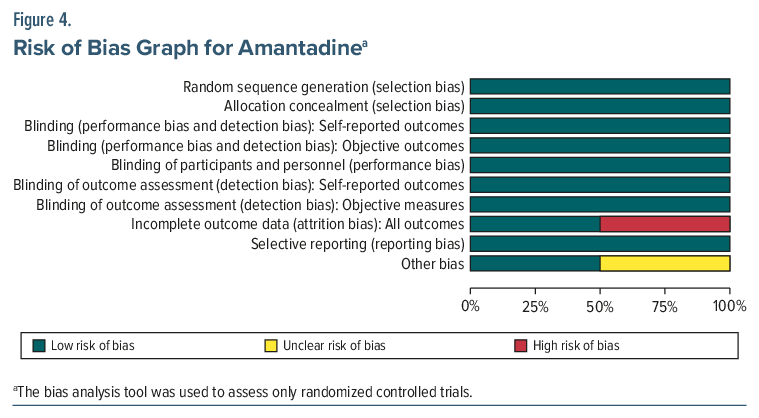
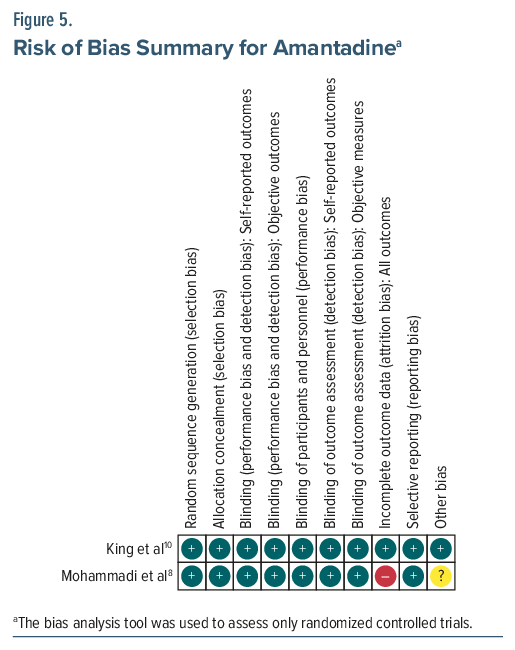
The methodological quality of the RCTs was evaluated using the Cochrane Collaboration’s risk-of-bias tool, which assesses selection, performance, detection, attrition, reporting, and other biases. Each bias category was rated as low, high, or unclear risk. Due to the limited number of studies, quantitative tests for assessing publication bias were not conducted.
The male-to-female ratio in the studies ranged from approximately 70% to 100%. The mean age of the participants was between 6 and 12 years, although 1 study included adults up to 26 years old. The duration of memantine treatment varied. In RCTs, treatment lasted between 10 and 48 weeks, while the open-label trial by Chez et al12 extended over 21 months. The retrospective cohort study by Morrow et al11 tracked participants for varying periods. Outcome measures also varied, with studies using different behavioral scales such as the Social Responsiveness Scale and the Aberrant Behavior Checklist-Community, as well as various assessments of language, memory, and IQ.
There was diversity in the formulations and administration routes used. Some trials used extended-release formulations of memantine, while others did not specify the formulation. Dosages ranged from 10 to 15 mg/day with different administration frequencies. For amantadine, treatment duration in RCTs ranged from 6 to 10 weeks, with dosages between 100 and 200 mg/day, administered once or twice daily. In summary, the studies reviewed exhibited considerable variability in their designs, treatment regimens, and outcome measures. Figures 2–5 provide the risk-of-bias analyses for the RCTs.
Memantine
Memantine, an uncompetitive NMDA receptor antagonist primarily approved for moderate to severe Alzheimer disease, has been investigated as a potential treatment for ASD due to its ability to modulate glutamatergic transmission. The glutamatergic system, particularly NMDA receptor-mediated excitatory neurotransmission, has been implicated in the pathophysiology of ASD. Dysregulated synaptic plasticity, excitotoxicity, and disrupted excitation-inhibition balance may underlie core features of ASD, including social impairments, repetitive behaviors, and cognitive rigidity. These neurobiological hypotheses have fueled interest in glutamate-modulating agents such as memantine; however, the current evidence base is limited, and findings are inconsistent.
One of the most comprehensive investigations of memantine’s efficacy was conducted by Aman et al,14 who performed a multisite RCT using an extended-release formulation of memantine in 121 children aged 6 to 12 years with a clinical diagnosis of ASD. Despite its scale, the trial failed to demonstrate significant improvements on the primary outcome measure, the Social Responsiveness Scale, when compared to placebo.14 Several design-related limitations undermine the interpretability of these negative findings. Nearly one-third of participants used prohibited medications during the study, and only 66 of 121 participants completed the protocol. The demographics were largely composed of white males, which further limits generalizability. Additionally, no information was collected on concurrent behavioral therapies or educational supports, making it difficult to isolate memantine’s specific pharmacologic impact.
Another randomized trial by Soorya et al16 investigated memantine in a more narrowly defined sample of verbally fluent children with ASD. This 24-week study reported modest gains in language, cognition, and memory, but its methodological limitations diminish confidence in these results. The trial was underpowered, with a total sample size of 23 and an attrition rate of 39%. Importantly, participants continued concurrent psychotropic treatments, including stimulants and antipsychotics, thus introducing significant confounding factors.16 The absence of a washout phase or control for polypharmacy raises questions about whether the observed improvements were attributable to memantine or to interactions with other medications.
A study by Hardan et al15 reviewed 3 phase 2 multicenter clinical trials assessing the safety and efficacy of memantine ER in children with ASD. The studies reviewed included a 50-week open-label trial, a randomized 12-week double-blind placebo-controlled withdrawal trial, and a 48-week open-label extension study. The studies primarily observed for improvements in the Social Responsiveness Scale and adverse effects or safety events. A change in the Social Responsiveness Scale of 10 points or greater was deemed to be clinically significant. The review did not meet its predetermined efficacy criteria in the double-blind trial but did show a statistically significant change in the open-label trial. None of the clinical trials displayed any evidence for safety concerns.15
Open-label studies, such as that by Chez et al,12 provide additional anecdotal support for memantine’s tolerability and possible utility in clinical practice. In this study, 151 individuals aged 2 to 26 years with ASD or pervasive developmental disorder not otherwise specified were treated with memantine while maintaining stable regimens of psychotropics, including selective serotonin reuptake inhibitors, stimulants, and antipsychotics. Reported improvements included gains in receptive language and reductions in stereotypies and irritability.12 However, the study lacked a control group, relied on caregiver-reported outcomes, and included a wide age and diagnostic range, thereby substantially limiting its internal validity. The open-label nature of the trial, combined with its subjective outcome measures and absence of blinding, increases susceptibility to placebo effects and expectancy bias.
More compelling evidence for memantine’s potential role emerges from a small but methodologically rigorous trial by Ghaleiha et al,13 which examined memantine as an adjunct to risperidone in the treatment of irritability in children with ASD. Over a 10-week period, 40 children were randomly assigned to receive risperidone with either memantine or placebo. The memantine augmentation group demonstrated significantly greater reductions in irritability scores on the Aberrant Behavior Checklist (ABC). The double-blind, placebo-controlled design strengthens the internal validity of the findings, and the adjunctive approach aligns with the growing consensus that glutamate modulators may exert their most beneficial effects in combination with agents targeting dopaminergic and serotonergic systems. However, the sample size was limited, and the study duration was short, raising concerns about statistical power and long-term safety.
Taken together, the existing body of evidence suggests that memantine is generally well tolerated in children and adolescents with ASD, but its clinical efficacy remains inconclusive. Findings from controlled trials have been mixed, with negative results in monotherapy settings and more promising outcomes when used adjunctively.
Amantadine
Amantadine, a glutamatergic modulator with dopaminergic properties, has been explored as a potential adjunctive treatment for irritability and hyperactivity in children with ASD. Its pharmacologic profile, including NMDA receptor antagonism and enhancement of dopamine release, makes it a theoretically appealing candidate for addressing core and associated symptoms of ASD, particularly those related to arousal dysregulation and behavioral rigidity. However, empirical evidence for its efficacy remains limited and inconsistent, warranting critical evaluation of existing studies.
An RCT by Mohammadi et al8 evaluated amantadine as an adjunct to risperidone in children aged 4 to 12 years with ASD who exhibited persistent irritability and hyperactivity. Participants were randomly assigned to receive risperidone with either amantadine or placebo over a 10-week period. Findings suggested significantly greater reductions in disruptive behaviors in the amantadine group. However, the sample was small and recruited from a single outpatient center, limiting external validity. No comprehensive information was provided regarding prior psychotropic exposures, and the 6-week discontinuation period for risperidone prior to randomization may not have been sufficient to eliminate carryover effects. Moreover, the study protocol intended to evaluate participants biweekly, but due to practical constraints, only 2 assessments were conducted across the entire trial, raising questions about the adequacy of outcome measurement and temporal resolution. Psychosocial interventions were not permitted during the study period, but the authors did not account for possible preexisting therapeutic supports, which could have confounded treatment response. Thus, while the results appear promising, the study’s internal and external validity is compromised by design limitations.8
In contrast, a smaller double-blind placebo-controlled trial by King et al10 assessed the tolerability and efficacy of amantadine monotherapy in 39 children and adolescents with ASD. Over a 6-week period, participants were administered either amantadine or placebo, with outcome measures including the Aberrant Behavior Checklist-Community Version (ABC-CV) and Clinical Global Impressions (CGI) scale. Although parent-rated outcomes did not significantly differ between groups, clinicians rated greater improvement in hyperactivity and irritability among those receiving amantadine. The discrepancy between parent and clinician ratings raises important questions about measurement reliability and potential observer bias. Additionally, the brief duration of the study and the relatively small, homogeneous sample limit the ability to generalize findings or detect sustained therapeutic effects. The exclusion of participants with comorbid conditions or lower intellectual functioning may also reduce ecological validity, given the heterogeneity inherent in ASD populations. This study, while methodologically more rigorous than some open-label reports, offers only tentative support for the use of amantadine and underscores the need for studies that integrate multiple informant perspectives across longer periods.
Further insight into amantadine’s potential utility emerges from a retrospective cohort analysis by Morrow et al,11 which reviewed the outcomes of 297 children prescribed amantadine for various psychiatric symptoms in a clinical setting. While over 60% of participants were reported to achieve clinically meaningful improvement and a sizable subset discontinued other psychotropic medications during treatment, the study’s retrospective and uncontrolled design introduces significant interpretive limitations. It is unclear which specific symptoms were targeted by treatment, and ASD was not consistently identified as the diagnostic focus. The heterogeneous sample, variability in treatment duration, and absence of structured outcome measures diminish the capacity to attribute observed benefits to amantadine or to discern its differential effects across diagnostic categories. Moreover, no data were provided regarding baseline symptom severity, comorbidities, or psychosocial interventions, all of which could substantially influence outcomes. While the study11 offers some support for amantadine’s tolerability and real-world use, it falls short of providing compelling evidence for its efficacy in ASD-specific contexts.
Similar to memantine, amantadine seems to exhibit favorable safety and tolerability profiles as well as potential evidence for benefit in hyperactivity and irritability, particularly in combination with antipsychotic medications. However, until more standardized data are available, its use should be considered experimental and reserved for treatment-refractory cases within the context of comprehensive, individualized care.
DISCUSSION
The systematic review of the literature on memantine and amantadine offers a nuanced perspective on their potential roles in the treatment of ASD. Both agents share mechanistic relevance to the neurobiology of ASD through modulation of glutamatergic and dopaminergic pathways. Memantine, an NMDA receptor antagonist, and amantadine, a dopaminergic agent with NMDA antagonistic properties, have been explored as pharmacologic interventions aimed at addressing core and associated symptoms of ASD. However, the available evidence remains inconclusive, characterized by small sample sizes, heterogeneity in study designs, and inconsistent outcome measures.
Despite mechanistic plausibility and generally favorable tolerability profiles, the evidence supporting either memantine or amantadine for ASD is currently preliminary and inconsistent. Across studies, core symptoms such as social communication deficits and restricted interests have not demonstrated reliable improvement with these agents. When benefits are observed, they appear limited to a subset of comorbid symptoms, including aggression, hyperactivity, and irritability. However, even in these domains, effect sizes are modest and often context dependent.
The level of evidence for both agents remains at Level 3 (Grade C) due to limitations in trial design, sample heterogeneity, and inconsistent replication. Importantly, no study to date has identified clear phenotypic or neurobiological subgroups that may preferentially benefit from either agent, which limits the application of these findings to precision medicine frameworks in ASD.17 Future research must incorporate biomarker stratification, neurocognitive endophenotyping, and longitudinal designs to determine whether specific subgroups, such as individuals with ASD and co-occurring ADHD, anxiety, or severe irritability, might benefit more consistently.
Across these studies, a central limitation is the lack of empirical precision in identifying which subgroups of individuals with ASD may benefit from these interventions. Trials to date have largely relied on broad categorical diagnoses, without examining stratification based on symptom clusters, cognitive profiles, neurobiological markers, or co-occurring psychiatric conditions. The absence of biotype-driven analyses leaves open the possibility that both memantine and amantadine may have utility in narrowly defined subpopulations—for example, children with ASD and high irritability, hyperactivity, or overlapping ADHD features—yet this hypothesis remains untested.
Moreover, the outcome measures employed in most trials focus heavily on parent-and clinician-rated scales, with minimal incorporation of objective or ecologically valid assessments. The ABC and CGI, while widely used, may not adequately capture subtle cognitive or social-emotional changes and are vulnerable to expectancy effects.18 This issue is compounded by the frequent exclusion of cointerventions (eg, behavioral therapies), limiting the ecological validity of findings. Few trials have evaluated long-term functional outcomes, such as adaptive behavior or quality of life, and the potential for cumulative effects remains unknown.
From a risk-benefit perspective, both agents appear to be generally well-tolerated, with side effects that are typically mild to moderate. Memantine has a favorable safety profile in pediatric populations, though its off-label use for ASD raises questions about long-term neurodevelopmental effects. Amantadine, with its dopaminergic effects, carries a slightly greater risk of activation, insomnia, and behavioral disinhibition, particularly in individuals with affective lability or seizure susceptibility. The risk of psychiatric side effects, including agitation or mood shifts, underscores the need for careful monitoring, especially when used in combination with other psychotropics.
Given the current state of evidence, routine use of memantine or amantadine for ASD cannot be broadly recommended. However, they may have situational utility as adjunctive agents in treatment-refractory cases, particularly when targeting specific behavioral symptoms such as irritability, aggression, or hyperactivity, and where standard treatments (eg, risperidone, aripiprazole) are contraindicated, poorly tolerated, or ineffective. In such cases, shared decision-making with families, close monitoring of target symptoms, and periodic reevaluation of efficacy and tolerability are essential.
In summary, while memantine and amantadine remain pharmacologically intriguing and well-tolerated, current data do not support their widespread clinical use for ASD without further confirmatory evidence. They may be considered in individualized treatment plans as adjunctive options for behavioral dysregulation, particularly when first-line agents are ineffective or poorly tolerated. However, clinicians should remain cautious, monitor for treatment-emergent side effects, and set realistic expectations regarding therapeutic outcomes.
Limitations
The current body of research on memantine and amantadine for ASD is limited by several methodological issues. Many studies suffer from small sample sizes, which reduce statistical power and increase the risk of false positives or negatives. Additionally, the lack of diversity in participant demographics, particularly the overrepresentation of white males, limits the generalizability of findings to broader populations, especially given the differential expression of ASD across sexes and ethnic groups.
A key limitation is the reliance on parent and clinician reports, which are subjective and prone to bias. More objective, multi-informant measures, including standardized functional assessments, are needed to evaluate the real-world efficacy of these medications. Furthermore, many studies had short durations, ranging from 6 to 48 weeks, which limits the ability to assess sustained treatment effects or the long-term benefits of these drugs.
The heterogeneity in study design, inclusion criteria, outcome measures, and concurrent treatments complicate cross-study comparisons and limit the strength of the overall evidence. Moreover, the reliance on short-term trials precludes conclusions about the sustainability of any observed benefits. The methodological rigor of existing studies varies widely, and the failure to account for developmental stage, intellectual functioning, or co-occurring conditions undermines the external validity of most findings.
Future research must address these limitations through larger, multisite randomized trials with clearly defined subgroups, stratified based on symptom dimensions, neurocognitive profiles, and biomarker correlates. Trials should also incorporate objective neurophysiological or neuroimaging end points to better elucidate potential mechanisms of action. Given the plausible neurobiological rationale and early adjunctive signals, memantine warrants continued investigation, but at present, it cannot be recommended as a standard treatment for ASD outside of carefully monitored research settings.
Another issue is the exclusion of concurrent psychosocial interventions, which are often standard in clinical practice. The lack of integration of these treatments in study protocols complicates understanding how pharmacologic agents interact with other therapeutic approaches. Moreover, the variability in trial designs, such as differences in participant age, outcome measures, dosing, and coadministration of other medications, makes it difficult to draw definitive conclusions across studies.
Finally, while safety data were generally positive, the small sample sizes and short follow-up periods prevent thorough assessment of long-term adverse effects, especially in subgroups such as young children or individuals with intellectual disabilities. In summary, while initial findings suggest potential benefits of memantine and amantadine for ASD, the methodological limitations in the current literature highlight the need for larger, more diverse, and methodologically rigorous studies to fully establish their clinical role.
CONCLUSION
The current evidence regarding the efficacy of memantine and amantadine in treating ASD is insufficient to draw definitive clinical conclusions. Although both medications exhibit favorable safety profiles, their effectiveness in addressing the core symptoms of ASD remains unproven. A critical limitation across studies is the methodological variability, including small sample sizes, lack of diverse participant representation, and inconsistent outcome measures. Additionally, many studies did not account for the potential impact of concurrent psychosocial interventions, which are typically integrated into standard clinical care but often excluded from research protocols.
Given the current lack of robust psychopharmacologic evidence for memantine and amantadine, these medications remain primarily off-label and should be considered cautiously in clinical settings. While they may offer potential benefits, particularly for managing comorbid symptoms such as irritability and aggression, their therapeutic role should be clearly defined through rigorous clinical research. The future of pharmacologic treatment for ASD lies in evidence-based, personalized approaches that integrate both pharmacologic and nonpharmacologic interventions.
FUTURE DIRECTIONS
To enhance the clinical relevance of future research, larger, multicenter RCTs are necessary to establish the generalizability and robustness of findings. These trials should include well-defined patient populations, with attention to the age, gender, and cultural diversity of participants. Moreover, utilizing standardized, multi-informant assessment protocols, incorporating both parent and clinician ratings, will help mitigate potential biases and offer a more comprehensive evaluation of treatment effects. Longer-duration studies (months to years) are particularly important to assess not only immediate symptom management but also sustained behavioral and developmental outcomes, which are crucial for long-term treatment planning. The phenotypes that appeared to have the greatest response were irritability, aggression, or hyperactivity, so focusing future studies on patients with these symptoms may be more responsive.
Additionally, it is vital to explore the interaction between pharmacologic treatments and psychosocial interventions, as they represent the cornerstone of ASD management in clinical practice. The exclusion of psychosocial treatments from many trials limits the ecological validity of the findings, as real-world treatment often combines medication with behavioral and educational therapies. Future studies should identify whether patients are receiving adjunct treatment to further assess the efficacy of concurrent pharmacologic or psychosocial interventions.
Article Information
Published Online: July 9, 2026. https://doi.org/10.4088/PCC.25r04152
© 2026 Physicians Postgraduate Press, Inc.
Submitted: November 26, 2025; accepted February 16, 2026.
To Cite: Gupta N, Parker N, Saeed A, et al. NMDA receptor antagonists in pediatric autism spectrum disorder: a systematic review. Prim Care Companion CNS Disord 2026;28(4):25r04152.
Author Affiliations: Wright State University, Dayton, Ohio (N. Gupta, Parker); Epionique Healthcare (N. Gupta); University of Cincinnati, Ohio (Saeed); Department of Psychology, Christ University, Delhi NCR, India (Khurana); University of Illinois Chicago, Illinois (Qureshi); Dayton Children’s Hospital, Dayton, Ohio (Emeronye); University of Texas, Austin, Texas (Gandhi); Northwestern University, Chicago, Illinois (Srinivasan); Loma Linda University, Loma Linda, California (M. Gupta).
Corresponding Author: Mayank Gupta, MD, Loma Linda University, Loma Linda, California ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
Clinical Points
- There is currently insufficient evidence for regular use of amantadine/memantine in autism spectrum disorder.
- Memantine and amantadine remain primarily off-label and should be considered cautiously in clinical settings.
References (18)

- Data and statistics on autism spectrum disorder. Autism Spectr Disord (ASD). 2025. Accessed April 28, 2025. https://www.cdc.gov/autism/data-research/index.html
- Hirota T, King BH. Autism spectrum disorder: a review. JAMA. 2023;329(2):157–168. PubMed CrossRef
- Gettu N, Saadabadi A. Aripiprazole. In: StatPearls. StatPearls Publishing; 2025. Accessed April 28, 2025. http://www.ncbi.nlm.nih.gov/books/NBK547739/
- McNeil SE, Gibbons JR, Cogburn M. Risperidone. In: StatPearls. StatPearls Publishing; 2025. Accessed April 28, 2025. http://www.ncbi.nlm.nih.gov/books/NBK459313/
- Montanari M, Martella G, Bonsi P, et al. Autism spectrum disorder: focus on glutamatergic neurotransmission. Int J Mol Sci. 2022;23(7):3861. PubMed CrossRef
- Siegel-Ramsay JE, Romaniuk L, Whalley HC, et al. Glutamate and functional connectivity - support for the excitatory-inhibitory imbalance hypothesis in autism spectrum disorders. Psychiatry Res Neuroimaging. 2021;313:111302. PubMed CrossRef
- Nisar S, Bhat AA, Masoodi T, et al. Genetics of glutamate and its receptors in autism spectrum disorder. Mol Psychiatry. 2022;27(5):2380–2392. PubMed CrossRef
- Mohammadi MR, Yadegari N, Hassanzadeh E, et al. Double-blind, placebo-controlled trial of risperidone plus amantadine in children with autism: a 10-week randomized study. Clin Neuropharmacol. 2013;36(6):179–184. PubMed CrossRef
- Brignell A, Marraffa C, Williams K, et al. Memantine for autism spectrum disorder. Cochrane Database Syst Rev. 2022;8(8):CD013845. PubMed
- King BH, Wright DM, Handen BL, et al. Double-blind, placebo-controlled study of amantadine hydrochloride in the treatment of children with autistic disorder. J Am Acad Child Adolesc Psychiatry. 2001;40(6):658–665. PubMed CrossRef
- Morrow K, Choi S, Young K, et al. Amantadine for the treatment of childhood and adolescent psychiatric symptoms. Proc Bayl Univ Med Cent. 2021;34(5):566–570. PubMed CrossRef
- Chez MG, Burton Q, Dowling T, et al. Memantine as adjunctive therapy in children diagnosed with autistic spectrum disorders: an observation of initial clinical response and maintenance tolerability. J Child Neurol. 2007;22(5):574–579. PubMed CrossRef
- Ghaleiha A, Asadabadi M, Mohammadi MR, et al. Memantine as adjunctive treatment to risperidone in children with autistic disorder: a randomized, double-blind, placebo-controlled trial. Int J Neuropsychopharmacol. 2013;16(4):783–789. PubMed CrossRef
- Aman MG, Findling RL, Hardan AY, et al. Safety and efficacy of memantine in children with autism: randomized, placebo-controlled study and open-label extension. J Child Adolesc Psychopharmacol. 2017;27(5):403–412. PubMed CrossRef
- Hardan AY, Hendren RL, Aman MG, et al. Efficacy and safety of memantine in children with autism spectrum disorder: results from three phase 2 multicenter studies. Autism Int J Res Pract. 2019;23(8):2096–2111. PubMed CrossRef
- Soorya LV, Fogg L, Ocampo E, et al. Neurocognitive outcomes from memantine: a pilot, double-blind, placebo-controlled trial in children with autism spectrum disorder. J Child Adolesc Psychopharmacol. 2021;31(7):475–484. PubMed CrossRef
- Dessus-Gilbert ML, Nourredine M, Zimmer L, et al. NMDA antagonist agents for the treatment of symptoms in autism spectrum disorder: a systematic review and meta-analysis. Front Pharmacol. 2024;15:1395867. PubMed CrossRef
- Schmidt JD, Huete JM, Fodstad JC, et al. An evaluation of the Aberrant Behavior Checklist for children under age 5. Res Dev Disabil. 2013;34(4):1190–1197. PubMed CrossRef
Please sign in or purchase this PDF for $40.