Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss the diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2026;28(3):25f04106
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Have you ever wondered how many people sustain an out-of-hospital cardiac arrest (OHCA) and how they manage to cope after it? Have you ever considered mood changes, such as depression, anxiety, and posttraumatic stress disorder (PTSD), which occur following a cardiac arrest? Have you been unsure about what treatment options might be available for psychosocial, cognitive, and community support for patients and their families following a cardiac arrest? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Mr A, a 66-year-old retired, but physically active, police officer with hypertension and hyperlipidemia, developed an acute onset of burning chest and shoulder pain while eating dinner. Initially, he attributed his symptoms to indigestion; however, persistent discomfort prompted concern in his spouse, and she encouraged him to go to the emergency department (ED) when his symptoms failed to resolve by bedtime. On arrival at the ED, he reported moderate chest pain, mild dyspnea, and diaphoresis. A 12-lead electrocardiogram demonstrated ST-segment elevation in leads II, III, and augmented vector foot, consistent with an inferior ST-elevation myocardial infarction (MI). Initial laboratory evaluation revealed an elevated cardiac troponin level and a mildly elevated white blood cell count. He was treated with aspirin and underwent an emergent percutaneous coronary intervention (PCI) to the right coronary artery within 90 minutes of his arrival. His hospital course was uncomplicated, and he was discharged home with close outpatient follow-up.
In the weeks following his hospital discharge, Mr A became increasingly anxious about the possibility of having another MI. During a visit with his primary care physician, his spouse expressed worries about his heightened vigilance related to bodily sensations and his persistent fear of having recurrent cardiac events. Mr A described that he had felt as though he was losing control during the emergent PCI, and he became reluctant to discuss anticipated retirement plans, including travel, due to his concerns about his cardiac health.
Roughly 1 month after his MI, Mr A collapsed while walking on a treadmill at his gym. Emergency medical services (EMS) were activated immediately, and cardiopulmonary resuscitation (CPR) was initiated by trained staff within 1 minute. An automated external defibrillator identified a shockable rhythm, and a single shock restored spontaneous circulation after approximately 4 minutes. On arrival to the ED, Mr A was drowsy but hemodynamically stable. He was treated with a beta-blocker, and he underwent implantation of an implantable cardioverter-defibrillator (ICD) for secondary prevention of sudden cardiac death (SCD). He tolerated the procedure well and was discharged home.
In the days to weeks following this hospital discharge, Mr A experienced significant anxiety, emotional lability, tearfulness, and a persistent fear that his heart “would stop again.” He avoided being alone, became hypervigilant to bodily sensations and hyperaware of ICD-related perceptions, and reported intrusive thoughts of his own mortality, disturbed sleep, avoidance of exercise, poor concentration, and difficulty reconnecting with his family and his identity as an active individual. Mr A’s spouse also became psychologically distressed, and she felt guilty about not being with him at the time of his cardiac arrest and anxious about his safety during routine activities. Although previously social and engaged, Mr A became increasingly withdrawn and disengaged from activities that he had previously enjoyed.
DISCUSSION
How Often Do People Sustain an OHCA?
More than 355,000 OHCAs occur in the United States each year, with an overall incidence of 81.3 per 100,000 person-years.1,2 OHCAs can be classified as having either medical (nontraumatic) or traumatic causes. According to estimates from the Cardiac Arrest Registry to Enhance Survival, EMS responded to more than 263,000 medical (nontraumatic) OHCAs in the United States in 2024, which corresponds to an incidence of 78.7 cases per 100,000 people, with substantial variation across states.3 Within medical OHCAs, drug-attributable OHCAs have emerged as a substantial and growing contributor in recent years and account for approximately 8% of nontraumatic OHCAs.3 In areas hardest hit by the opioid crisis, drug-attributable OHCA rates as high as 17.6% of nontraumatic OHCAs have been reported.4 In contrast, traumatic OHCAs, defined as cardiac arrests that result from external physical injury (eg, blunt or penetrating trauma, drowning, electrocution, or asphyxiation), are typically analyzed separately because of the important differences in epidemiology, etiology, pathophysiology, management, and survival. Traumatic OHCAs occur less frequently than nontraumatic OHCAs and account for approximately 3.2% of all reported OHCAs.5
What Causes Sudden Cardiac Arrest?
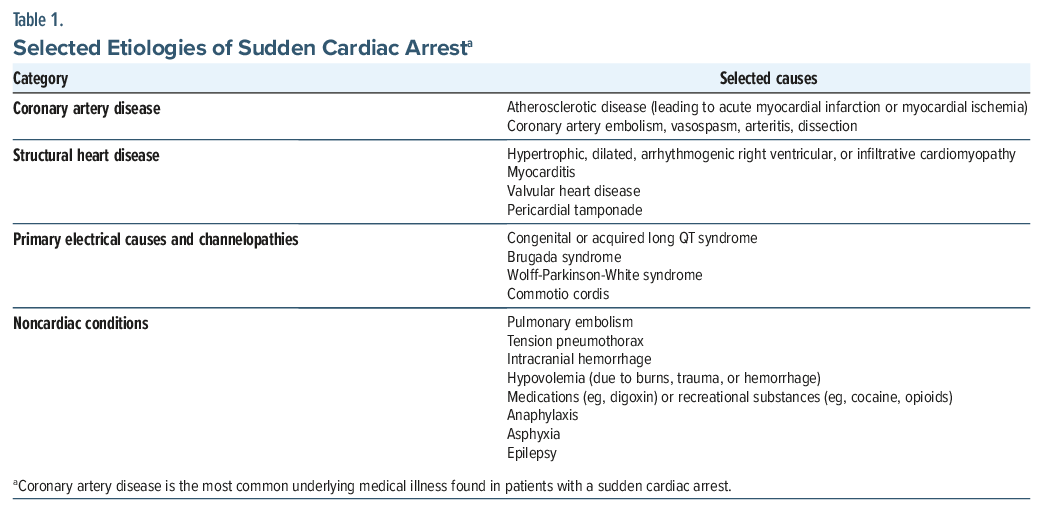
Sudden cardiac arrest (SCA) may result from both cardiac and noncardiac conditions (see Table 1 for selected etiologies).5–8 Cardiac etiologies account for most of the hospital presentations for OHCAs, with one retrospective cohort study showing that more than half of cases had a primary cardiac cause.5,8 Coronary artery disease (CAD) is the most common cause of SCA, implicated in approximately three-fourths (70%–75%) of SCDs, especially in the first few months after acute MI.9,10 This increase in the rate after MI is due to ventricular or myocardial scar tissue formation that results in slowed conduction in some myocardial areas, creating an environment favorable to the genesis of arrhythmias.10 Other common cardiac causes include structural heart disease (eg, cardiomyopathies, myocarditis, valvular heart disease, and pericardial tamponade) and primary electrical disorders or channelopathies (eg, congenital or acquired long QT syndrome, Brugada syndrome, Wolff-Parkinson-White syndrome, and complete heart block).6,7 Among patients with cardiac etiologies, most OHCAs are precipitated by ventricular arrhythmias (eg, ventricular fibrillation [VF], polymorphic ventricular tachycardia [VT]) and complete heart block or pulseless electrical activity (PEA).10–13 Noncardiac causes of SCA (eg, pulmonary embolism, asphyxiation, and recreational substance use) also cause ventricular arrhythmias or PEA.
Several risk factors increase one’s susceptibility to SCA and can be categorized as genetic, behavioral, and medical. A family history of SCD significantly elevates one’s risk of OHCA, underscoring the role of genetic predisposition and heritable diseases.14 Male sex and advanced age are also independently associated with higher rates of OHCA.3 Behavioral factors (eg, cigarette smoking, physical inactivity, and drug use) are notable contributors,15 with current tobacco use, a lack of regular exercise, substance use, and drug overdose strongly associated with an increased risk of OHCA.14,15
Medical comorbidities, such as hypertension, hyperlipidemia, chronic kidney disease (CKD), congestive heart failure (CHF), and HIV infection, significantly increase one’s risk of experiencing an arrhythmia and SCA through various mechanisms.16 Hypertension contributes to atherosclerosis, which can lead to ischemia and an increased risk of arrhythmia. Elevated lipid levels promote plaque formation, resulting in systemic inflammation and myocardial ischemia and further increasing the risk of arrhythmias. CKD can lead to arrhythmia-promoting electrolyte imbalances and has synergistic worsening effects on cardiovascular illness with hypertension and hyperlipidemia. CHF weakens the heart, decreasing its efficiency and making it more susceptible to developing an arrhythmia. In HIV infection, certain retroviral treatments can lead to metabolic syndrome, compounding cardiovascular risks. A meta-analysis has shown that cardiac causes remain the most common etiology of SCA across all ages; in younger individuals, congenital cardiac disease and noncardiac causes (eg, drug toxicity and congenital abnormalities) are comparatively more prevalent, whereas in older adults, CAD represents the dominant risk factor for SCA.15,17
What Determines the Survival Rate of Those Who Sustain an OHCA?
Overall survival following an OHCA remains low and varies substantially by the arrest’s etiology. In general, when someone has sustained a nontraumatic, presumed cardiac OHCA, they have a significantly greater survival rate.8 Survival after hospital discharge following a medical (nontraumatic), presumed cardiac OHCA is approximately 10%,3 whereas survival following a traumatic OHCA varies, with a reported survival range of 4%–30%.3,8 Among medical OHCAs, survival is higher for those with an drug-attributable OHCA compared with those having other causes (15.2% vs 6.9%).3
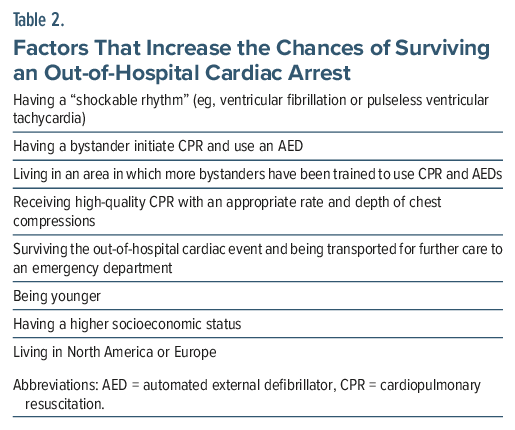
Survival after an OHCA is influenced by multiple interrelated factors, including whether the arrest was bystander-witnessed, the time from collapse to EMS arrival, the prompt initiation of CPR, the initial cardiac rhythm, the patient’s age, and the presence of premorbid medical and neurological comorbidities (Table 2).18–22 The subgroup with the highest likelihood of survival involves patients who had a bystander-witnessed OHCA with a presumed cardiac etiology and an initial “shockable” rhythm, specifically VF or pulseless VT.18 Patients in this category also have the most favorable neurological outcomes.19
Patient-specific characteristics further modify prognosis. Younger age and shorter intervals between collapse and EMS arrival are associated with improved survival rates.18 In contrast, several comorbid medical conditions (eg, diabetes mellitus, peripheral arterial disease, hypertension, and a right bundle branch block) are associated with a lower likelihood of survival.18,20 Older age and certain sociodemographic factors, including one’s ethnic background, have also been associated with worse outcomes following an OHCA.18,20
How Efficacious Is CPR, and What Types of Sequelae Can Individuals Sustain Following CPR?
CPR is a lifesaving intervention; however, it is associated with both acute physical injuries and potential long-term neurological sequelae. The most common acute complications of CPR are fractures of the ribs and sternum, which can cause significant chest wall pain as well as potential pulmonary problems.23 Injuries to intra-abdominal organs, although less frequent, have also been reported. A recent systematic review found that traumatic injuries to the liver and spleen occurred in up to 15% of cases (with one study showing a rate of 29% when mechanical compressions were administered), while ischemic injuries (eg, of the liver, intestines, and mesenteric network) were even more common and consistently linked to a higher mortality rate.24 These findings emphasize the need to monitor for abdominal complications in individuals with an unexplained postresuscitation deterioration.
Beyond structural injuries, the most serious sequelae of CPR are neurological problems. Post–cardiac arrest brain injury (PCABI) arises from global cerebral ischemia during the cardiac arrest and from reperfusion injuries that follow the return of spontaneous circulation. PCABI is the leading driver of outcomes among survivors, associated with high rates of mortality and long-term neuropsychiatric sequelae (eg, impaired consciousness, depression, PTSD, and anxiety).25 Predictors of the neurological outcome include the initial rhythm (shockable vs nonshockable), witnessed versus unwitnessed cardiac arrest, and physiological variables that include cerebral oxygenation and reperfusion dynamics.25 Sekhon and colleagues25 stressed the heterogeneity of PCABI and the need for further research to better predict prognosis and to guide targeted therapies.
What, If Anything, Do Survivors of a Cardiac Arrest Recall About Their Experience and Resuscitation?
Although cardiac arrest leads to the abrupt cessation of perfusion and oxygen delivery to the brain, causing immediate metabolic changes and loss of consciousness (LOC) within seconds to minutes, some patients report recollections or experiences of their resuscitation.26 There is a growing literature base on near-death experiences (NDEs) and recalled experiences of death (REDs) after cardiac arrest.27–29 Both are provoked by life-threatening encounters and often result in spiritual experiences that appear to mitigate the fear of death. REDs, a more recently described phenomenon, involve structured, lucid, cognitive, and emotional experiences that form a narrative arc during the period of presumed LOC.29 Those who reported experiencing a RED during their cardiac arrest often recall it as transcendental, transformative, and an overall positive experience.28,29 One study of patients who experienced a cardiac arrest and who underwent CPR attempted to map the physiological underpinnings of REDs, showing near-normal electroencephalographic activity consistent with consciousness and potential resumption of organized cortical activity up to 1 hour into CPR.28 Despite this expanding literature, reports of NDEs and REDs post–cardiac arrest are uncommon, though this may be because of the survivors’ fear of not being taken seriously.
How Do People React to Having Their ICD Fire?
Patients describe the sensation of receiving a high-energy ICD shock in myriad ways, although most commonly it has been described as a feeling like a sudden, forceful blow to the chest that is accompanied by moderate-to-severe chest pain, sometimes with an electrical quality.30 The most frequent initial psychological response to an ICD-delivered shock is anxiety, which is often followed by relief that the abnormal rhythm was detected and treated, as well as uncertainty regarding the risk of a recurrent arrhythmia, additional shocks, or the need for an urgent medical evaluation.31 Following a shock, many patients experience somatic symptoms of anxiety (eg, diaphoresis, tachycardia, tachypnea, and muscle tension), which are frequently triggered by device-related concerns (eg, of device malfunction, impending death, and ongoing shocks).31 Feelings of demoralization, despondency, and depression are also common, as the shock may serve as a reminder of personal vulnerability and mortality.31
Although most individuals who have received an ICD feel reassured by having the device, some patients develop intense psychological distress, including depression (20%), anxiety (30%), and avoidance behaviors of activities that are perceived as physiologically stressful.31 Elevated rates of PTSD symptoms have been documented among those with a variety of cardiovascular conditions, with prevalence estimates reaching 12% in those who have had an ICD placed, a rate that is substantially higher than that found in the general population and equal to the rates of PTSD recorded in US Army veterans.31,32 Notably, approximately one-fifth of individuals with an automatic implantable cardioverter-defibrillator met the criteria for PTSD at their initial evaluation, suggesting that prior severe cardiovascular illnesses may confer preexisting psychological vulnerability.33 Rates are even higher among survivors of an OHCA, with the prevalence of PTSD approaching 38% at their initial assessment.33 A minority of ICD recipients report experiencing phantom shocks, that is, the perception of an ICD shock in the absence of device-recorded therapy.34 Phantom shocks appear to occur more frequently among individuals with co-occurring mood symptoms.35
What Types of Affective, Behavioral, and Cognitive Changes Might Survivors of a Cardiac Arrest Develop?
Most survivors of a cardiac arrest report that the experience changed their life. Although some survivors experience long-term positive changes following their resuscitation, many develop long-term affective, behavioral, and cognitive sequelae. These outcomes are thought to arise from a combination of an anoxic brain injury sustained during the arrest36 and the immediate and ongoing emotional toll of having sudden, enduring losses in cognitive and physical function, as well as a heightened sense of vulnerability to death (ie, mortality salience).37 The presence of an anoxic brain injury is associated with worse psychosocial outcomes, including higher rates of depression, anxiety, and PTSD.36
Anxiety, PTSD, and depression are common among survivors of a cardiac arrest and appear to endure long term.38,39 Notably, post–cardiac arrest PTSD often appears to be maintained less by recollection of the arrest itself than by enduring somatic threat, including recurrent bodily sensations and daily reminders of the arrest and its sequelae.37,40 Such reminders often include ICD sensations, pain related to resuscitative interventions, postarrest fatigue, or heightened interoceptive awareness of cardiac function. PTSD symptoms following cardiac arrest are strongly correlated with comorbid anxiety and depression, impaired concentration ability, increased somatic complaints, and pessimism regarding one’s prognosis, which reflects a broader experience of emotional distress.27
Anxiety is particularly prominent following a cardiac arrest and often manifests as fear of recurrence, hypervigilance, and excessive monitoring of cardiac symptoms. Younger age, a history of generalized anxiety, a history of a heart murmur, and a history of at least 1 ICD shock are associated with an increased risk of developing cardiac anxiety.41 Individuals with cardiac anxiety are more likely to avoid physical activity, report higher cardiovascular disease–related distress, perceive worse health outcomes, and endorse greater functional disability.41
Affective disorders following cardiac arrest are not only prevalent but also clinically consequential. Anxiety, depression, and PTSD have each been associated with worse long-term outcomes. In a large population-based cohort study, survivors with anxiety or depression had a 1.41-fold and 1.44-fold greater risk of long-term mortality, respectively, compared with survivors without these conditions.42 Another study demonstrated that screening positive for PTSD at hospital discharge was linked to a 3.1-fold increased risk of major adverse cardiovascular events and all-cause mortality within 1 year.43 Secondary analyses suggested that symptoms of hyperarousal (particularly insomnia) drove this association.44 Sleep disturbances are common in survivors of a cardiac arrest and may occur in the context of affective disorders or due to the fear of dying while asleep.45 Collectively, these findings underscore the importance of identifying and treating psychological distress to optimize long-term outcomes following a cardiac arrest.
In addition to affective and behavioral changes, cognitive impairment is common following a cardiac arrest. Survivors may exhibit deficits in long-term memory, focal cognitive domains, and executive function.27 Specific impairments have been documented in working memory, delayed free recall, prose recall, and prospective memory, whereas short-term memory assessed via free recall and recognition performance remains comparable to population norms.46 These cognitive changes may increase vulnerability to later neurodegenerative processes, including Alzheimer disease.47 Certain brain areas (eg, watershed regions, areas supplied by end arteries, regions with high metabolic and oxygen demand, and those densely populated with glutaminergic neurons) are exceptionally sensitive to cardiac arrest due to hypoxia.36
What Types of Psychological Support Are Available for Those Who Survive a Cardiac Arrest?
Survivors of an SCA often require multidisciplinary care that addresses both the medical drivers of recurrence and its psychological aftermath. While the American Heart Association recommends referral for psychological support,48 the optimal therapeutic modalities for this population have not yet been established definitively. Emerging evidence suggests that cognitive-behavioral therapy (CBT)–informed interventions and dyadic interventions that involve both the survivor and their primary family caregiver may be beneficial,49–53 although there is still an absence of robust large-scale efficacy and effectiveness trials. These approaches target maladaptive cognitions and behaviors related to cardiac arrest and recovery, including catastrophic thinking, hypervigilance to bodily sensations, and avoidance of physical activity. Core components often include promoting cognitive appraisal or defusion, diaphragmatic breathing, mindfulness, acceptance, value-based living, behavioral activation, sleep hygiene, and structured psychoeducation with anticipatory guidance regarding common challenges during recovery.49,50 Interventions may also include preparation for and response planning around ICD shocks.49,50
In addition to psychotherapy, comprehensive, multidisciplinary cardiac rehabilitation programs that integrate psychological support show promise in improving fatigue, physical functioning, and quality of life.54–58 Equally important are peer-support networks and survivor communities, which can provide ongoing counseling, emotional support, education, and connection.59,60 Such programs may complement formal clinical interventions, help reduce isolation, foster resilience, and promote long-term adjustment.
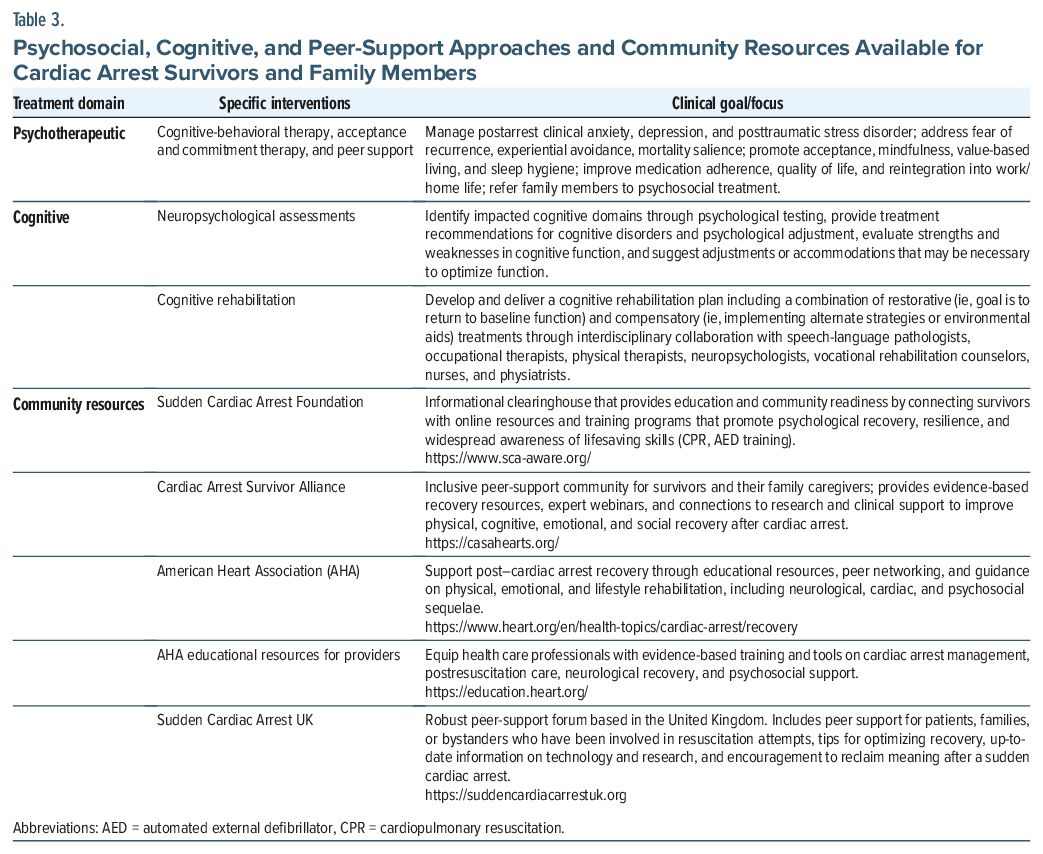
Resources for patients, families, and providers, including evidence-based training and continuing education, are summarized in Table 3.
What Types of Interventions Can Help Family Members of Those Who Have Sustained a Cardiac Arrest?
Family members of those who have sustained a cardiac arrest frequently experience significant psychological distress including anxiety, depression, and PTSD. They often struggle with uncertainty regarding their loved one’s prognosis and with the abrupt transition into a caregiving role following hospital discharge. Approximately 15%–30% of family members screen positive for caregiver burden, and many report inadequate information or insufficient support to meet caregiving demands.60–64 Among those who witnessed the cardiac arrest, heightened vigilance and overprotective behaviors are common, often accompanied by neglect of their own physical and emotional needs.65
Recognizing this burden, the American Heart Association recommends psychosocial screening and referral to family members of cardiac arrest survivors,48 despite relatively few interventional studies. Two early pilot interventions demonstrated the feasibility and acceptability of providing caregiver support shortly after a cardiac arrest,53,66 while one randomized controlled trial showed improved outcomes for both survivors and caregivers when both participated together in a structured psychosocial nursing intervention, compared with survivor-only participation.51
In the absence of extensive interventional trials, qualitative studies of family caregivers and a systematic review and meta-analysis have generated practical recommendations for family support.67 Immediately following the cardiac arrest, families benefit from receiving clear, consistent information regarding the suspected cause of the arrest, the resuscitative efforts undertaken, who provided care, and what to expect in the days to weeks ahead.67 Delivering this information both verbally and in plainly written materials empowers families to ask informed questions and prepares them for a range of possible outcomes.67 Assignment of a dedicated hospital point person to provide ongoing communication and emotional support is recommended, as is acknowledging and validating family distress.67 Families also benefit from access to basic hospital amenities, including spaces to rest, bathe, charge electronic devices, and grieve.67 For bereaved family members, reassurance that their loved one did not suffer and that resuscitative efforts were exhausted may provide meaningful comfort.67 Before hospital discharge, families benefit from opportunities for peer support and from screening for psychological distress.65,67 Postdischarge follow-up for family members (regardless of the patient’s outcome) by medical social workers is strongly encouraged as it can facilitate case management, address caregiving challenges, and identify emerging mental health needs.65
Whether family members should be present during the resuscitation (either in-hospital or out-of-hospital) remains an area of ongoing debate. The 2023 International Liaison Committee on Resuscitation Guidelines suggest that family members be offered the option of being present during adult resuscitation.68 This recommendation is based on a lack of evidence of harm to patients or families due to family presence and the potential for benefits for both parties. The guidelines further emphasize the importance of training health care professionals to manage both family distress and their own emotional responses during these high-intensity events.68
What Happened to Mr A?
Mr A’s family encouraged him to make an appointment with a psychologist for ongoing concerns about his mood. Psychotherapeutic interventions included mindfulness and relaxation strategies for the management of his physiological arousal and anticipatory anxiety, as well as CBT that focused on recognizing and reframing catastrophic thoughts, rebuilding a sense of normalcy and self-efficacy, and managing identity loss. Mr A’s psychologist encouraged him to connect with an online cardiac arrest survivor community and encouraged family counseling to help his spouse process her fears that might hinder Mr A’s autonomy. By his 6-month follow-up visit, Mr A had returned to his hobbies and was participating in a low-intensity exercise program. His ICD had not discharged. He continued taking beta-blockers that resulted in his having a stable blood pressure and no further arrhythmias. Psychologically, he showed marked improvement; however, he described intermittent anxiety, especially before medical appointments or device interrogations. Mood scales showed mild residual symptoms, but they were not suggestive of a major mood episode.
CONCLUSION
OHCA is one of the leading causes of death around the world. OHCA is caused by arrhythmias (eg, VT, VF, or PEA) that may result from many illnesses, but most are cardiac causes. Survival rates for those who have sustained an OHCA are low overall but vary depending on both medical and patient-specific factors. Although some survivors of a cardiac arrest experience joy and peace during the event, many others experience enduring affective and cognitive challenges postarrest that require specialty care.
Article Information
Published Online: June 4, 2026. https://doi.org/10.4088/PCC.25f04106
© 2026 Physicians Postgraduate Press, Inc.
Submitted: October 10, 2025; accepted January 30, 2026.
To Cite: DeSimone AC, Presciutti AM, Braford MB, et al. Improving cardiac arrest survivorship: managing mental health of survivors and family members. Prim Care Companion CNS Disord 2026;28(3):25f04106.
Author Affiliations: Department of Psychiatry, Bayhealth Medical Center, Dover, Delaware (DeSimone); Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts (Presciutti, Matta, Stern); Department of Psychiatry, Harvard Medical School in Boston, Massachusetts (Presciutti, Matta, Stern); Lewis Gale Medical Center in Salem, Virginia (Braford, Mastronardi); Department of Psychiatry, McGill University Health Care Center, Montreal, Canada (Ibrahim); Department of Psychiatry, Michigan Medicine, University of Michigan, Ann Arbor, Michigan (Rosinski); Home Base an affiliate of Massachusetts General Hospital, Boston, Massachusetts (Matta).
DeSimone, Presciutti, Braford, Mastronardi, Ibrahim, Rosinski, and Matta are co-first authors; Stern is the senior author.
Corresponding Author: Sofia E. Matta, MD, Department of Psychiatry, Massachusetts General Hospital, Harvard Medical School, 55 Fruit St, Boston, MA 02114
([email protected]).
Financial Disclosure: Dr Presciutti is a scientific advisor to the Sudden Cardiac Arrest Foundation and the Cardiac Arrest Survivor Alliance. Dr Stern has received royalties from Elsevier for editing textbooks on psychiatry. Drs DeSimone, Braford, Mastronardi, Ibrahim, Rosinski, and Matta have no disclosures or conflicts of interest.
Funding/Support: None.
Clinical Points
- Survival rates of those who suffer an out-of-hospital cardiac arrest depend upon the time from the onset of cardiac arrest to the arrival of emergency medical services and the initiation of cardiopulmonary resuscitation, the individual’s age, and the presence of comorbid medical and neurological conditions. However, the most reliable predictor of survival is the presence of an initial “shockable rhythm” (eg, ventricular fibrillation or a pulseless ventricular tachycardia).
- The most common initial psychological response after an implantable cardioverter-defibrillator–delivered shock is anxiety with prominent physical manifestations of anxiety; this is often followed by both relief and uncertainty.
- Affective states and conditions (eg, anxiety, posttraumatic stress disorder, and depression) are common in those who have survived a cardiac arrest, and untreated psychiatric symptoms are associated with worse cardiac outcomes.
- Psychosocial, cognitive, and peer support services are available for patients, caregivers, bystanders, and clinicians.
References (68)

- Ghzally Y, Mahajan K. Implantable defibrillator. In: StatPearls [Internet]. StatPearls Publishing; 2025. http://www.ncbi.nlm.nih.gov/books/NBK459196/
- McBride O, Poel A, Counts CR, et al. Temporal patterns in out-of-hospital cardiac arrest incidence and outcome. JAMA Cardiol. 2025;10(9):922–931. CrossRef
- CARES - cardiac arrest registry to Enhance survival - 2024 Annual report [Internet]. https://mycares.net/sitepages/uploads/2025/2024_flipbook/index.html?page=66
- Wang RC, Montoy JCC, Rodriguez RM, et al. Trends in presumed drug overdose out-of-hospital cardiac arrests in San Francisco, 2015–2023. Resuscitation. 2024;198:110159. CrossRef
- Gässler H, Fischer M, Wnent J, et al. Outcome after pre-hospital cardiac arrest in accordance with underlying cause. Resuscitation. 2019 May;138:36–41. PubMed CrossRef
- Myat A, Song KJ, Rea T. Out-of-hospital cardiac arrest: current concepts. Lancet. 2018 Mar;391(10124):970–979. PubMed CrossRef
- Stiles MK, Wilde AAM, Abrams DJ, et al. 2020 APHRS/HRS expert consensus statement on the investigation of decedents with sudden unexplained death and patients with sudden cardiac arrest, and of their families. Heart Rhythm. 2021;18(1):e1–e50. CrossRef
- Wittwer MR, Zeitz C, Beltrame JF, et al. Aetiology of resuscitated out-of-hospital cardiac arrest treated at hospital. Resuscitation. 2022;170:178–183. CrossRef
- Centers for Disease Control and Prevention (CDC). State-specific mortality from sudden cardiac death-United States, 1999. MMWR Morb Mortal Wkly Rep. 2002;51(6):123–126. PubMed
- Frampton J, Ortengren AR, Zeitler EP. Arrhythmias after acute myocardial infarction. Yale J Biol Med. 2023;96(1):83–94. PubMed CrossRef
- Link MS, Bockstall K, Weinstock J, et al. Ventricular tachyarrhythmias in patients with hypertrophic cardiomyopathy and defibrillators: Triggers, treatment, and implications. J Cardiovasc Electrophysiol. 2017;28(5):531–537. PubMed CrossRef
- Speranzon A, Chicco D, Bonazza P, et al. Brugada syndrome: Focus for the general pediatrician. Children. 2024;11(3):281. PubMed CrossRef
- Pereira AR, Briosa A, Miranda R, et al. Sudden cardiac death: the most feared but potentially preventable presentation of Wolff-Parkinson-White syndrome. In: Sciarra L, ed. Case Rep Cardiol;2021:1–6.
- Jung E, Park JH, Ro YS, et al. Family history, socioeconomic factors, comorbidities, health behaviors, and the risk of sudden cardiac arrest. Sci Rep. 2023;13(1):21341. PubMed CrossRef
- Paratz ED, Van Heusden A, Zentner D, et al. Causes, circumstances, and potential preventability of cardiac arrest in the young: insights from a state-wide clinical and forensic registry. EP Eur. 2022;24(12):1933–1941. CrossRef
- Thorgeirsson G, Thorgeirsson G, Sigvaldason H, et al. Risk factors for out-of-hospital cardiac arrest: the Reykjavik Study. Eur Heart J. 2005;26(15):1499–1505. PubMed CrossRef
- Yan S, Gan Y, Jiang N, et al. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care Lond Engl. 2020;24(1):61. PubMed CrossRef
- Matta A, Philippe J, Nader V, et al. Predictors and rate of survival after out-of-hospital cardiac arrest. Curr Probl Cardiol. 2024;49(9):102719. PubMed CrossRef
- Chan PS, McNally B, Tang F, et al. Recent trends in survival from out-of-hospital cardiac arrest in the United States. Circulation. 2014;130(21):1876–1882. PubMed CrossRef
- Goto Y, Funada A, Maeda T, et al. Sex-specific differences in survival after out-of-hospital cardiac arrest: a nationwide, population-based observational study. Crit Care. 2019;23(1):263. PubMed CrossRef
- Nagraj S, Varrias D, Kharawala A, et al. Ethnic and sex-based differences in outcomes after out-of-hospital cardiac arrest: a glimpse of the largest municipal healthcare system in the United States. Cardiovasc Diagn Ther. 2023;13(1):1–10. PubMed CrossRef
- Sasson C, Rogers MAM, Dahl J, et al. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3(1):63–81. PubMed CrossRef
- Van Wijck SFM, Prins JTH, Verhofstad MHJ, et al. Rib fractures and other injuries after cardiopulmonary resuscitation for non-traumatic cardiac arrest: a systematic review and meta-analysis. Eur J Trauma Emerg Surg. 2024;50(4):1331–1346. PubMed CrossRef
- Hoftun FB, Hagemo J, Rehn M. Abdominal organ injury in cardiac arrest: systematic literature review. Nik Ab. Rahman NH. PLOS One. 2025;20(8):e0329164. PubMed
- Sekhon MS, Taccone FS, Skrifvars MB, et al. Clinical heterogeneity and phenotyping of post cardiac arrest brain injury: one size may not fit all. Intensive Care Med. 2025;51(7):1240–1255. PubMed CrossRef
- Sekhon MS, Ainslie PN, Griesdale DE. Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: a “two-hit” model. Crit Care. 2017;21(1):90. PubMed CrossRef
- Parnia S, Spearpoint K, Fenwick PB. Near death experiences, cognitive function and psychological outcomes of surviving cardiac arrest. Resuscitation. 2007;74(2):215–221. PubMed CrossRef
- Parnia S, Keshavarz Shirazi T, Patel J, et al. AWAreness during REsuscitation - II: a multi-center study of consciousness and awareness in cardiac arrest. Resuscitation. 2023;191:109903. PubMed CrossRef
- Parnia S, Post SG, Lee MT, et al. Guidelines and standards for the study of death and recalled experiences of death––a multidisciplinary consensus statement and proposed future directions. Ann N Y Acad Sci. 2022;1511(1):5–21. PubMed CrossRef
- Dunbar SB, Warner CD, Purcell JA. Internal cardioverter defibrillator device discharge: experiences of patients and family members. Heart Lung J Crit Care. 1993;22(6):494–501. PubMed
- Ghezzi ES, Sharman RLS, Selvanayagam JB, et al. Burden of mood symptoms and disorders in implantable cardioverter defibrillator patients: a systematic review and meta-analysis of 39 954 patients. Europace. 2023;25(6):euad130. PubMed CrossRef
- Hoge CW, Riviere LA, Wilk JE, et al. The prevalence of post-traumatic stress disorder (PTSD) in US combat soldiers: a head-to-head comparison of DSM-5 versus DSM-IV-TR symptom criteria with the PTSD checklist. Lancet Psychiatry. 2014;1(4):269–277. PubMed CrossRef
- Ladwig KH, Baumert J, Marten-Mittag B, et al. Posttraumatic stress symptoms and predicted mortality in patients with implantable cardioverter-defibrillators: results from the prospective living with an implanted cardioverter-defibrillator study. Arch Gen Psychiatry. 2008;65(11):1324–1330. PubMed CrossRef
- Jacob S, Panaich SS, Zalawadiya SK, et al. Phantom shocks unmasked: clinical data and proposed mechanism of memory reactivation of past traumatic shocks in patients with implantable cardioverter defibrillators. J Interv Card Electrophysiol. 2012;34(2):205–213. PubMed CrossRef
- Prudente LA, Reigle J, Bourguignon C, et al. Psychological indices and phantom shocks in patients with ICD. J Interv Card Electrophysiol. 2006;15(3):185–190. PubMed CrossRef
- Perez CA, Samudra N, Aiyagari V. Cognitive and functional consequence of cardiac arrest. Curr Neurol Neurosci Rep. 2016;16(8):70. PubMed CrossRef
- Presciutti A, Siry-Bove B, Newman MM, et al. Qualitative study of long-term cardiac arrest survivors’ challenges and recommendations for improving survivorship. J Am Heart Assoc. 2022;11(14):e025713. PubMed CrossRef
- Chen X, Li D, He L, et al. The prevalence of anxiety and depression in cardiac arrest survivors: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2023;83:8–19. PubMed CrossRef
- Presciutti A, Newman MM, Vranceanu AM, et al. Associations between depression and anxiety symptoms with quality of life in cardiac arrest survivors with good neurologic recovery and informal caregivers of cardiac arrest survivors. J Affect Disord Rep. 2020;2:100046. PubMed CrossRef
- Presciutti AM, Bannon SM, Yamin JB, et al. The relationship between mindfulness and enduring somatic threat severity in long-term cardiac arrest survivors. J Behav Med. 2023;46(5):890–896. PubMed CrossRef
- Rosman L, Whited A, Lampert R, et al. Cardiac anxiety after sudden cardiac arrest: severity, predictors and clinical implications. Int J Cardiol. 2015;181:73–76. PubMed CrossRef
- Lee J, Cho Y, Oh J, et al. Analysis of anxiety or depression and long-term mortality among survivors of out-of-hospital cardiac arrest. JAMA Netw Open. 2023;6(4):e237809. PubMed CrossRef
- Agarwal S, Presciutti A, Cornelius T, et al. Cardiac arrest and subsequent hospitalization–induced posttraumatic stress is associated with 1-year risk of major adverse cardiovascular events and all-cause mortality. Crit Care Med. 2019;47(6):e502–e505. PubMed CrossRef
- Presciutti A, Shaffer J, Sumner JA, et al. Hyperarousal symptoms in survivors of cardiac arrest are associated with 13-month risk of major adverse cardiovascular events and all-cause mortality. Ann Behav Med. 2020;54(6):413–422. PubMed CrossRef
- Hellström A, Bremer A, Gunnarsson L, et al. Sleep in cardiac arrest survivors. Nurs Crit Care. 2023;28(6):870–877. PubMed CrossRef
- Sulzgruber P, Kliegel A, Wandaller C, et al. Survivors of cardiac arrest with good neurological outcome show considerable impairments of memory functioning. Resuscitation. 2015;88:120–125. PubMed CrossRef
- Secher N, Adelborg K, Szentkúti P, et al. Evaluation of neurologic and psychiatric outcomes after hospital discharge among adult survivors of cardiac arrest. JAMA Netw Open. 2022;5(5):e2213546. PubMed CrossRef
- Hirsch KG, Amorim E, Coppler PJ, et al Part 11: post–cardiac arrest care: 2025 American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2025;152(16_suppl_2). S673, S718. PubMed
- Ford J, Rosman L, Wuensch K, et al. Cognitive–behavioral treatment of posttraumatic stress in patients with implantable cardioverter defibrillators: results from a randomized controlled trial. J Trauma Stress. 2016;29(4):388–392. PubMed CrossRef
- Bergman M, Markowitz JC, Kronish IM, et al Acceptance and mindfulness-based exposure therapy for PTSD after cardiac arrest: an open feasibility trial. J Clin Psychiatry. 2024;85(1):23m14883.
- Dougherty CM, Thompson EA, Kudenchuk PJ. Patient plus partner trial: a randomized controlled trial of 2 interventions to improve outcomes after an initial implantable cardioverter-defibrillator. Heart Rhythm. 2019;16(3):453–459. PubMed CrossRef
- Auld JP, Thompson EA, Dougherty CM. Social cognitive intervention following an initial implantable cardioverter defibrillator: better treatment response for secondary versus primary prevention. Pacing Clin Electrophysiol. 2020;43(9):974–982. PubMed CrossRef
- Presciutti AM, La Camera D, Perman SM, et al. Single-arm feasibility trial of a resilience intervention for cardiac arrest survivors and their family caregivers, Recovering together after cardiac arrest. Resuscitation. 2025;216:110855. PubMed CrossRef
- Joshi VL, Tang LH, Kim YJ, et al. Promising results from a residential rehabilitation intervention focused on fatigue and the secondary psychological and physical consequences of cardiac arrest: the SCARF feasibility study. Resuscitation. 2022;173:12–22. PubMed CrossRef
- Singh KN, Baird S, Singh HN, et al. The outcomes of cardiac rehabilitation in out-of-hospital cardiac arrest – a narrative review. Contemp Nurse. 2025;61(6): 615–631. PubMed CrossRef
- Salwa K, Kaziród-Wolski K, Rębak D, et al. Current perspectives on rehabilitation following return of spontaneous circulation after sudden cardiac arrest: a narrative review. Healthcare. 2025;13(15):1865. PubMed CrossRef
- Moulaert VRM, Van Heugten CM, Winkens B, et al. Early neurologically-focused follow-up after cardiac arrest improves quality of life at one year: a randomised controlled trial. Int J Cardiol. 2015;193:8–16. PubMed CrossRef
- Kim YJ, Rogers JC, Raina KD, et al. An intervention for cardiac arrest survivors with chronic fatigue: a feasibility study with preliminary outcomes. Resuscitation. 2016;105:109–115. PubMed CrossRef
- Sawyer KN, Brown F, Christensen R, et al. Surviving sudden cardiac arrest: a pilot qualitative survey study of survivors. Ther Hypothermia Temp Manag. 2016;6(2):76–84. PubMed CrossRef
- Presciutti AM, Perman SM, Vranceanu AM. Mental health services in postcardiac arrest care. Neurocrit Care. 2024;41(3):715–718. PubMed CrossRef
- Bohm M, Cronberg T, Årestedt K, et al. Caregiver burden and health-related quality of life amongst caregivers of out-of-hospital cardiac arrest survivors. Resuscitation. 2021;167:118–127. PubMed CrossRef
- Van Wijnen HG, Rasquin SM, Van Heugten CM, et al. The impact of cardiac arrest on the long-term wellbeing and caregiver burden of family caregivers: a prospective cohort study. Clin Rehabil. 2017:31(9):1267–1275. PubMed CrossRef
- Beesems SG, Wittebrood KM, De Haan RJ, et al. Cognitive function and quality of life after successful resuscitation from cardiac arrest. Resuscitation. 2014;85(9):1269–1274. PubMed CrossRef
- Wachelder EM, Moulaert VRMP, Van Heugten C, et al. Life after survival: long-term daily functioning and quality of life after an out-of-hospital cardiac arrest. Resuscitation. 2009;80(5):517–522. PubMed CrossRef
- Rojas DA, DeForge CE, Abukhadra SL, et al. Family experiences and health outcomes following a loved ones’ hospital discharge or death after cardiac arrest: a scoping review. Resusc Plus. 2023;14:100370. PubMed CrossRef
- Cornelius T, Mendieta M, Cumella RM, et al. Family-authored ICU diaries to reduce fear in patients experiencing a cardiac arrest (FAID fear): a pilot randomized controlled trial. PLOS One. 2023;18(7):e0288436. PubMed CrossRef
- Douma MJ, Myhre C, Ali S, et al. What are the care needs of families experiencing sudden cardiac arrest? A survivor- and family-performed systematic review, qualitative meta-synthesis, and clinical practice recommendations. J Emerg Nurs. 2023;49(6):912–950. PubMed CrossRef
- Berg KM, Bray JE, Ng KC, et al. 2023 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: Summary from the basic life support; advanced life support; Pediatric life support; Neonatal life support; education, Implementation, and Teams; and first Aid Task Forces. Resuscitation. 2024;195:109992. PubMed
Please sign in or purchase this PDF for $40.




