Guillain-Barre syndrome (GBS) is an immune-mediated polyneuropathy often triggered by infection. Involvement of respiratory muscles can lead to respiratory failure and mechanical ventilation in 30% and 20% of cases, respectively.1 Extubation in patients with GBS is complicated by several factors, including the degree of respiratory muscle weakness2 and symptoms of anxiety. The latter has been determined to prolong mechanical ventilation weaning.3 We present the case of a patient with GBS, whose mechanical ventilation weaning was prolonged, in part, by “anxiety.”
Case Report
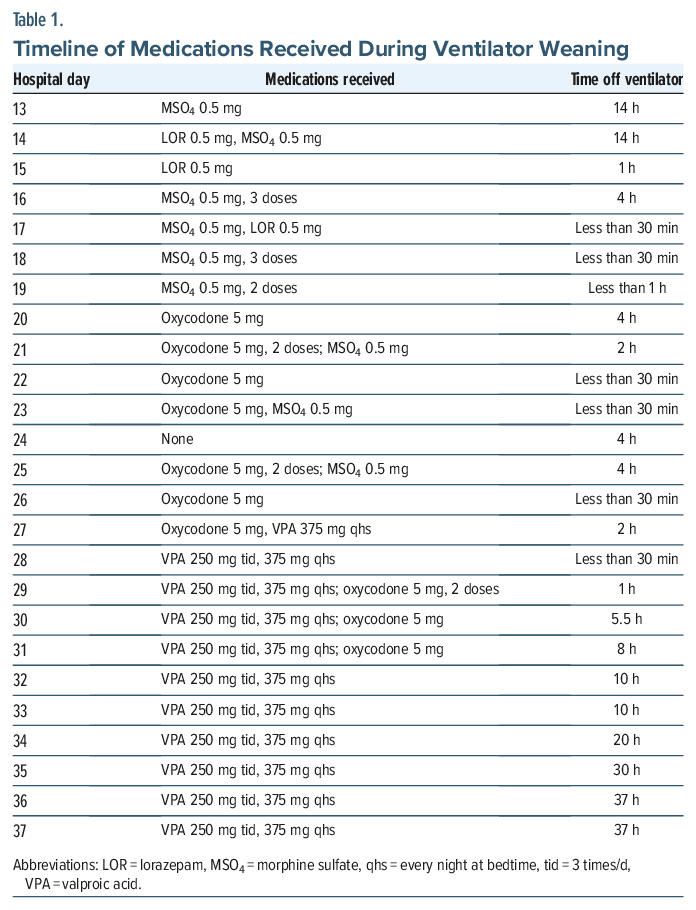
The patient was a 69-year-old man with a history of hyperlipidemia, hypertension, and GBS. He was admitted to our hospital’s extended recovery (ExR) section after being transferred from acute care for relapse of GBS. In acute care, the patient received 5 courses of intravenous immunoglobulin and 7 exchanges of plasmapheresis. He was intubated for impending respiratory failure and status post-tracheostomy. Admission ExR medications included atorvastatin 20 mg/day for hyperlipidemia, hydrochlorothiazide 25 mg/day for hypertension, omeprazole 40 mg/day for gastroesophageal reflux disease, rivaroxaban 20 mg/day for anticoagulation, and valsartan 160 mg/day for hypertension. On paraclinical evaluation, complete blood count/metabolic profile, thyroid function, and infectious workup were unremarkable. Physical examination was unremarkable with a neurological examination remarkable for bilateral upper extremity = 2/5, lower extremity strength = 0/5, and areflexia. Table 1 and Figure 1 provide spontaneous breathing trial (SBT) treatment and outcomes.2
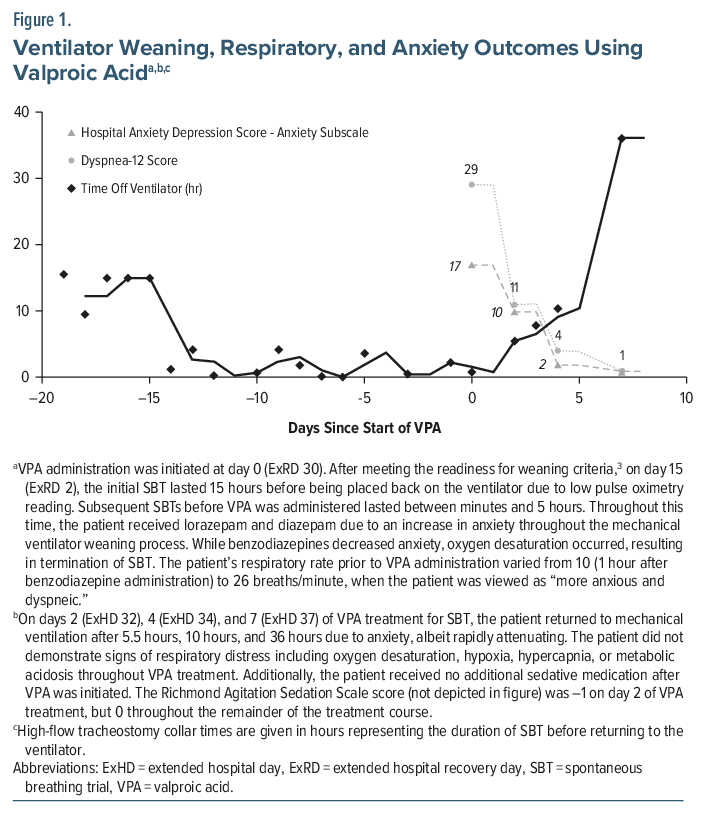
On ExR day (ExRD) 28, the psychiatry consult team was notified to request alternative medications to assist with SBT. The patient and his wife denied a prior psychiatric or substance/alcohol use history. The mental status examination was unremarkable except for anxious mood, but the patient denied psychotic/lethal ideations. The patient was oriented x 3. The Confusion Assessment Method for the Intensive Care Unit4 was negative for delirium. The patient’s Dyspnea-12 questionnaire (D-12)5 score was 29, while the Hospital Anxiety and Depression Scale (HADS)6 score was 25, with depression/anxiety subscale scores of 8 and 17, respectively. The Richmond Agitation Sedation Scale (RASS) score was 0.4
At this time, the patient was started on valproic acid (VPA) immediate release 250 mg 3 times/day, 375 mg at bedtime. On ExRD 30, 31, and 37, D-12 scores were 11, 4, and 1, respectively; HADS-Anxiety scores were 10, 2, and 1, respectively; RASS scores were –1, 0, and 0, respectively; and SBT durations were 5.5, 10.5, and 36 hours, respectively. Serum VPA level on hospital day 37 was 37 mcg/mL without blood dyscrasias or changes in the complete metabolic profile, lipase, or vital signs, including oxygen saturation. On hospital day 39, the patient was successfully transferred to a high-flow tracheostomy collar (HFTC), with D-12, HADS-Anxiety, and RASS scores remaining unchanged. Notably, the patient did not receive further benzodiazepines or dexmedetomidine or any other sedating after VPA was initiated.
Discussion
GBS often involves respiratory muscles and the oropharyngeal system, which can result in respiratory failure, with more than one-third of patients having anxiety at admission to the intensive care unit.7 Although benzodiazepines can be used as anxiolytics and sedation, randomized controlled trials have shown worse outcomes, including oversedation, delayed initiation, and prolonged mechanical ventilation.8–11 Our patient was treated with both lorazepam and diazepam before VPA was started. Other than the second day of VPA treatment, when the RASS score was –1, our patient’s RASS score was 0 throughout the treatment.
VPA is a broad-spectrum anticonvulsant that has demonstrated acute anxiolytic properties in healthy patients.12 While not devoid of respiratory depression, in head-to-head comparisons with benzodiazepines13 and in studies of patients with respiratory/neuromuscular disease, VPA has not demonstrated significant adverse respiratory outcomes.14,15 While dosing strategies for initiating VPA can vary,16 we administered VPA 4 times/day for potential maximal anxiolysis, as Tmax is 3.3 hours.17
Our patient’s response to VPA was consistent with the evidence base that, at low-to-moderate dosing, there was lack of respiratory depression. Furthermore, our patient’s ability to transition to HFTC within 10 days demonstrated potential efficacy in VPA for mechanical ventilation weaning. Nonetheless, we recommend further large-scale, randomized placebo-controlled studies utilizing VPA as the treatment for mechanical ventilation weaning in those with GBS and anxiety.
Article Information
Published Online: May 28, 2026. https://doi.org/10.4088/PCC.25cr04120
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(3):25cr04120
Submitted: October 28, 2025; accepted January 26, 2026.
To Cite: Spiegel DR, LaFever A, Vazquetelles R, et al. Prolonged mechanical ventilation weaning in a patient with Guillain-Barre syndrome, complicated by anxiety, treated successfully with valproic acid. Prim Care Companion CNS Disord 2026;28(3):25cr04120.
Author Affiliations: Department of Psychiatry and Behavioral Sciences, Macon and Joan Brock Virginia Health Sciences Eastern Virginia Medical School at Old Dominion University, Norfolk, Virginia (Spiegel, Lafever, Vazquetelles, Dorney); Georgetown University School of Medicine, Washington, DC (Sabet).
Corresponding Author: David R. Spiegel, MD, Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, 825 Fairfax Avenue, Norfolk, Virginia 23507 ([email protected]).
Financial Disclosure: None.
Funding/Support: Dr Spiegel is a member of the speaker’s bureau for AbbVie, Alkermes, and Intra-Cellular but has no conflicts of interest in the preparation of this manuscript.The remaining authors have no disclaimer/conflicts of interest to report.
Patient Consent: Consent was received from the patient to publish the case report, and information has been de-identified to protect anonymity.
References (17)

- Weiss N, Marois C, Le Guennec L, et al. Critical insights for intensivists on Guillain-Barré syndrome. Ann Intensive Care. 2025;15(1):67. PubMed CrossRef
- Watson V, Ghishan S, Avalishvili T, et al. Exploring Extubation readiness in Guillain-Barré syndrome: a case report and Literature review. J Investig Med High Impact Case Rep. 2025;13:23247096251331859. PubMed CrossRef
- Trudzinski FC, Neetz B, Dahlhoff JC, et al. A multidimensional approach to the management of patients in prolonged weaning from mechanical ventilation: the concept of treatable traits - a narrative review. Respiration. 2025; 104(4):240–254. PubMed CrossRef
- Ely EW, Margolin R, Francis J, et al. Evaluation of delirium in critically ill patients: validation of the confusion assessment method for the intensive care unit (CAM-ICU). Crit Care Med. 2001;29(7):1370–1379. PubMed CrossRef
- Yorke J, Moosavi SH, Shuldham C, et al. Quantification of dyspnoea using descriptors: development and initial testing of the Dyspnoea-12. Thorax. 2010;65(1):21–26. PubMed CrossRef
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. PubMed CrossRef
- Rajabally YA, Seri S, Cavanna AE. Neuropsychiatric manifestations in inflammatory neuropathies: a systematic review. Muscle Nerve. 2016;54(1):1–8. PubMed CrossRef
- Pearson SD, Patel BK. Evolving targets for sedation during mechanical ventilation. Curr Opin Crit Care. 2020;26(1):47–52. PubMed CrossRef
- Quickfall D, Sklar MC, Tomlinson G, et al. The influence of drugs used for sedation during mechanical ventilation on respiratory pattern during unassisted breathing and assisted mechanical ventilation: a physiological systematic review and meta-analysis. EClinicalMedicine. 2024;68:102417. PubMed CrossRef
- Boles JM, Bion J, Connors A, et al. Weaning from mechanical ventilation. Eur Respir J. 2007;29(5):1033–1056. PubMed CrossRef
- Pham T, Heunks L, Bellani G, et al. WEAN SAFE Investigators. Weaning from mechanical ventilation in intensive care units across 50 countries (WEAN SAFE): a multicentre, prospective, observational cohort study. Lancet Respir Med. 2023;11(5):465–476. PubMed CrossRef
- Bach DR, Korn CW, Vunder J, et al. Effect of valproate and pregabalin on human anxiety-like behaviour in a randomised controlled trial. Transl Psychiatry. 2018;8(1):157. PubMed CrossRef
- Prasad M, Krishnan PR, Sequeira R, et al. Anticonvulsant therapy for status epilepticus. Cochrane Database Syst Rev. 2014;2014(9):CD003723. PubMed CrossRef
- Antoniou T, Yao Z, Camacho X, et al. Safety of valproic acid in patients with chronic obstructive pulmonary disease: a population-based cohort study. Pharmacoepidemiol Drug Saf. 2015;24(3):256–261. PubMed CrossRef
- Elshafay A, Hieu TH, Doheim MF, et al. Efficacy and safety of valproic acid for spinal muscular atrophy: a systematic review and meta-analysis. CNS Drug. 2019;33(3):239–250. PubMed CrossRef
- https://www.pdr.net/drug-summary/?drugLabelId=Depakene-valproic-acid-979#dosage-and-indications
- Delage C, Palayer M, Etain B, et al. Valproate, divalproex, valpromide: are the differences in indications justified?. Biomed Pharmacother. 2023;158:114051. PubMed CrossRef
Please sign in or purchase this PDF for $40.