Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2026;28(4):25f04104
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Have you ever felt frustrated while attempting to communicate with an intubated patient? Have you wondered how you could enhance your ability to understand what your patients were trying to tell you? Have you been uncertain whether there are technologic tools that can clarify your patients’ needs? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Ms A, a 72-year-old woman with peripheral vascular disease, emphysema (requiring home oxygen), type 2 diabetes, hypertension, and a hearing impairment, was admitted to the intensive care unit (ICU) for acute-on-chronic respiratory failure that required intubation and mechanical ventilation. The psychiatry service was consulted to assist with management of anxiety and agitation that interfered with her care. On interview, Ms A tried repeatedly to speak, despite the presence of her endotracheal (ET) tube; unfortunately, neither her ICU team nor her family could understand what she was saying. Her escalating anxiety and restlessness contributed to repeated failures to wean her from the ventilator, which led the ICU team to consider placing a tracheostomy tube if she could not be extubated.
DISCUSSION
What Can Interfere With Effective Communication in Intubated Patients?
Patients in the ICU often struggle to communicate effectively, given anatomical and physical barriers, ICU-specific barriers, and cognitive and emotional factors. Moreover, interviews with ICU survivors suggest that impaired communication severely exacerbates both physical and psychological discomfort.1 Not only does impaired communication interfere with an individual’s ability to convey their basic needs, but it also thwarts the expression of their acute distress, which exacerbates their fears and predisposes to develop long-term sequelae.2,3 Despite the prevalence of these outcomes, ICU staff typically receive little training about how to communicate with intubated patients.2
What Types of Anatomical and Physiological Barriers to Communication Can Arise in Critically Ill Patients?
The most direct challenge to communication among mechanically ventilated individuals stems from the placement of an ET tube. Normal speech production begins with vibration of the vocal cords and the creation of sound, which is then amplified in the upper airways (eg, nose, mouth, and throat) and articulated through the lips, soft palate, and tongue. The diaphragm, lungs, and chest wall are also actively involved in phonation.4 Placement of an ET tube leads to airflow obstruction and impedance of vocal cord vibration, rendering the patient unable to speak.5,6 For patients with more chronic ventilatory requirements, a tracheostomy may be required. By repositioning the artificial airway from the mouth to the anterior aspect of the neck, the patient can mouth words and emote through facial expressions. However, they remain unable to produce speech due to the presence of a tracheostomy tube, which leads to similar physiological barriers as those caused by the ET tube.
Additional physiological complications that interfere with communication stem from ICU-acquired weakness, which can result in systemic or distributed weakness to limit facial expressions or physical gestures.3 Alternately, patients may become agitated and dislodge critical life-support equipment, which may require use of physical restraints that tether the wrists or encompass the patients’ hands.7 These interventions further limit efforts to communicate through gestures or writing. In addition, individuals who usually use dentures and who are without them in the ICU can develop communication difficulties due to alterations in the contour of their mouth that hinders proper vocalization of certain words.3
Which ICU-Specific Barriers to Communication Can Arise in Critically Ill Patients?
ICUs are stimuli-rich environments that are characterized by intrusive noises, lights, and instrumentation. These conditions often hinder staff’s ability to recognize and respond to patient cues, which results in patients’ frustration and distress.8,9 Subjective patient distress may be regarded by the ICU team as being due to critical life support interventions and may lead to use of higher doses of sedatives, analgesics, or neuromuscular blockades to calm and control patients. However, even therapeutic effects of these agents can impair a patient’s motor and cognitive abilities, which adversely impacts their speech and thought process.3 Moreover, deep sedation can worsen outcomes, such as the duration of being ventilated and the length of stay (LOS) in the ICU, which further complicates meaningful patient communication. Light sedation strategies lead to patients being more alert and cooperative, which expedites weaning from mechanical ventilation and shortens hospital LOS. Unfortunately, as ventilated patients become more engaged with their environment, they are often more likely to become frustrated, demoralized, and agitated.10
Addressing impaired communication with critically ill patients is a resource-intensive process that requires significant time, effort, and frequently a trial-and-error approach. Clinical staff cannot always expend the time required to commit to such personalized communication, and families may be reluctant to engage in this endeavor for fear of disrupting their loved ones’ clinical stability. Thus, the patient’s attempts to communicate may be dismissed as being indecipherable until their critical illness has abated.
Which Cognitive and Emotional Barriers to Communication Can Arise in Critically Ill Patients?
Delirium, demoralization, anxiety, and agitation are highly prevalent among intubated patients, and each can adversely impact short-and long-term outcomes among critically ill patients. In fact, anxiety, agitation, and pain were the most commonly cited reasons why patients failed the Spontaneous Awakening Trial (SAT) safety screen or the SAT itself.11 Other communication barriers faced in ICUs include language or cultural barriers or preexisting cognitive or functional impairment (eg, deficits in strength, coordination, vision, hearing).12 Moreover, critically ill patients are more likely to develop delusions (sometimes referred to as “delusional memories”) or fixed false beliefs, which may persist even after resolution of their critical illness and neurocognitive sequelae (eg, delirium). Such delusions occur in roughly two-thirds (68%) of critically ill patients who required mechanical ventilation and can cause long-lasting anxiety, paranoia, or depression among ICU survivors.13,14 By maintaining a high index of suspicion for these conditions, intensivists can systematically screen patients for relevant symptoms and intervene in a timely and effective fashion (often with information, clarification, reassurance, and administration of antipsychotic medications), while communicating to patients that they are being heard and that their concerns are being addressed. These interventions can both individually and synergistically reduce the patient’s distress as it directly relates to the experience of such symptoms.
Case Vignette, Continued
On psychiatric evaluation, Ms A was intubated and connected to mechanical ventilation; she was lying in bed with her eyes closed. When her arm was touched gently, she opened her eyes quickly and appeared afraid. The psychiatric consultant calmly introduced himself and explained that he was there to help her feel better. When the examiner asked Ms A to nod her head to signify “yes,” Ms A nodded, and the examiner commented, “I see that you are nodding your head. I can understand you clearly.” Ms A was instructed to answer questions by nodding her head vertically (for “yes”) and laterally (for “no”). The examiner limited his evaluation to using “yes” and “no” questions to gather information. On further questioning, the examiner learned that Ms A was unaware that she was in the hospital or that she had a breathing tube down her throat, limiting her ability to speak. The examiner reoriented Ms A by explaining, “You’re in the hospital” and “You have a breathing tube in your mouth and down your throat that is helping you breathe.” The evaluator also told Ms A that her wrists were being restrained so that she did not inadvertently pull out any tubes or lines. The examiner performed additional nonverbal cognitive testing to obtain additional information related to anxiety, dysphoria, pain, dyspnea, and insomnia; she endorsed insomnia, anxiety, and pain (in her back and in her throat). The evaluator then asked Ms A if anything strange or frightening had been happening to or around her, to which she nodded her head vigorously, suggesting the presence of delusions. The examiner reassured Ms A that she was safe and that everyone was taking good care of her. Then, he summarized Ms A’s status for her, stating that she was experiencing insomnia, anxiety, pain, and distress about her safety and that the psychiatric consultant planned to work with her primary team to improve her symptoms. Ms A’s family observed the examiner’s interactions with Ms A and was encouraged to provide similar efforts at reorientation and reassurance several times each day. They were also educated about delusions, delirium, early mobilization, and strategies they could use, such as “get to know me” boards and “ICU diaries,” so that they could support Ms A’s recovery using evidence-based approaches.
Which Strategies Can Enhance Communication With Intubated Patients?
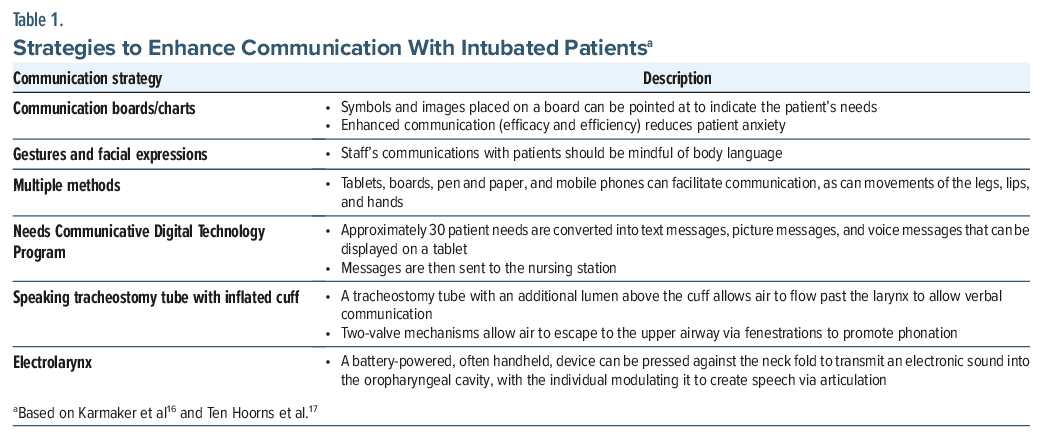
Clinicians who are familiar with several simple strategies and tools can facilitate effective communication with patients across multiple domains, focusing on the individuals’ wants and needs to ensure that their care reflects the sentiment “Nothing about me without me.”15 Since fluctuations in patients’ physical status, cognitive abilities (eg, due to delirium), and psychological experience (eg, associated with agitation, anxiety, and delusions) may limit engagement with communication devices or strategies, it is helpful to employ a multifaceted approach (Table 1).16,17 Clinicians may consider using augmentative and alternative communication (AAC) strategies that span the technology spectrum (ie, no-technology, low-technology, and high-technology approaches), tailoring their approach to each patient’s needs and abilities.18
What Are Some “No-Technology” Approaches to Enhance Communication?
To communicate effectively with intubated patients, clinicians should go beyond the standard question-and-answer format used in other clinical environments. Instead, an approach that prioritizes simplicity, positive engagement, and regular affirmation of the patient can be effective.19 This approach centers around the use of spoken and nonverbal communication (NVC) strategies, eg, making direct eye contact, holding the patient’s hands, and conveying a kind demeanor.20 Optimizing the environment can also facilitate a patient’s expression and understanding (eg, adjusting the lighting, decreasing background noise, providing access to eyeglasses and hearing aids, and providing access to the nursing call bell). Alternatively, it can be useful to communicate with a simple head nod/shake, eye blink, hand squeeze, or gesture (eg, thumbs-up/thumbs-down sign). Assessment of the patient’s communication abilities can begin by determining effective communication strategies, as determined by the patent’s motor abilities (eg, head nodding, thumbs up or down, blinking, or directing eye movements). Once a strategy has been established, the clinician should ask simple, closed-ended questions that require a “yes” or “no” response. Questions should be asked one at a time, and ample time should be given for the patient to respond. After each response or set of related responses, the clinician should summarize what was communicated to reassure the patient that their concerns were being addressed and to invite the correction of mistakes. Using this approach, patients often feel valued, understood, and experience hope.21
What Are Some “Low-Technology” Approaches to Enhance Communication?
Low-technology AACs can help patients indicate their needs and preferences (eg, using communication boards or other tools, such as picture boards, alphabet boards, or writing instruments). Communication boards with large fonts can be especially helpful for those with visual impairment. For those with limited English proficiency, it is important to provide communication boards and visual aids that are available in the patient’s preferred language. If writing instruments are used, the patient’s positioning should be optimized to ensure that they can see the writing surface and hold the pen or marker without interference from tethering lines or restraints. Patients may find it easier to write with a large marker than a smaller caliber pen or pencil. Some low-tech communication strategies require the assistance of others; therefore, providers and family members should be trained to use these tools so that they can be used throughout the day. When caring for individuals with intellectual disability or those who are challenged by verbal communication at baseline, collaboration with their caregivers can ensure that familiar communication boards are available at the bedside.
What Are Some “High-Technology” Approaches to Enhance Communication?
High-technology AACs include communication applications on tablet devices, speech-generating software, and voice output communication aids (VOCAs).22 A gaze-controlled, computer-assisted communication study of ICU patients found that such tools improved communication, with lower levels of anxiety.23 Gaze boards that use eye-tracking technology have the added advantage of being able to be used in patients who are unable to use their hands to communicate, although the technology may work better for patients with a lighter iris color compared with a darker color. The use of such eye-tracking software has improved clinicians’ ability to understand patient needs and improved the rate at which pain and depressive symptoms were identified.24 Other high-tech strategies use computer, tablet, or smartphone keyboards in lieu of more conventional writing utensils, as the higher-fidelity letter-to-screen interface reduces ambiguity on the part of the examiner, thus improving the efficiency and efficacy of patient communication. Incorporating AACs ultimately depends on a critically ill patient’s level of sedation, their physical and cognitive status, their psychological state, and the available resources within the health system that is providing care.25
What Are Some “Tracheostomy-Specific Strategies” That Enhance Communication?
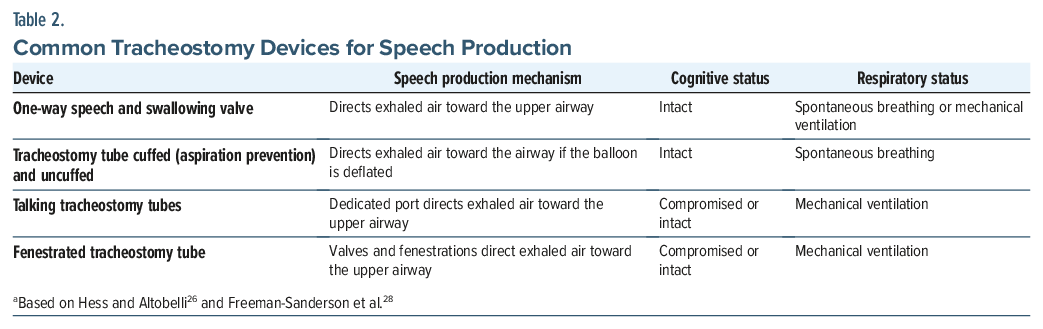
While patients who require the short-or long-term use of a tracheostomy can mouth words or emote more freely via making facial expressions, alternative strategies for communication can enhance and supplement meaningful communication (Table 2).26 Speech-language pathologists can evaluate patients who require a tracheostomy to determine if they can use speech augmentation aids, beginning with early cuff deflation trials.27 If a patient can tolerate a one-way valve, optimizing trans-laryngeal airflow aids in the recovery of their speech, swallowing, coughing, and self-expression.27 While the use of the one-way valve was historically reserved for patients no longer requiring mechanical ventilation, a randomized clinical trial comparing early use of the one-way speaking valve with those who were not permitted to use the valve until fully weaned off mechanical ventilation demonstrated that early valve use allowed patients to speak 11 days earlier than patients in the control arm.28 Earlier speech permitted more meaningful engagement by patients, allowing them to actively participate in their own care and leading to improved overall quality of life and reported mood symptoms.28 For those who cannot tolerate cuff deflation, above-cuff vocalization provides an alternative to speech production.29 With fenestrated tracheostomy tubes, air can move from the tracheostomy tube to the subglottic area toward the larynx, enabling speech when the cuff is inflated or partially inflated.30 Many individuals with a permanent tracheostomy learn to place their finger over the opening of the deflated cuff, or use a cuffless tracheostomy, to direct air through the upper airway to produce speech.26,31
While lip reading can be challenging for those who are unfamiliar with the practice, several strategies can improve the likelihood of understanding the patient’s communication efforts. Patients should be encouraged to speak slowly and clearly, while emphasizing their speech movements for important words.32 Care providers should observe how the patient moves their lips, jaw, and tongue and identify patterns in the lip movements that are made while speaking. In addition, the patient’s facial expressions often convey emotional tonality. Their body language can include fluctuations in eye contact and gestures used to communicate a specific message. Health care providers should ask for clarification to confirm that they understand what the patient has attempted to express. By starting with simple words and phrases, the assessment can become more complex after the provider understands the patient’s concerns. Using a whiteboard while lip reading can reduce the likelihood of misunderstandings between the patient and team members.
For non–English-speaking patients with a tracheostomy, the use of in-person interpreters can greatly facilitate communication, although the interpreter may require additional guidance on lip-reading strategies if the patient is not yet eligible for the use of a speaking valve. Interpreters can also assist in communicating with non–English-speaking family members to obtain valuable collateral information about the patient or to provide friends and family with helpful strategies to facilitate ICU liberation. Identifying cultural differences in communication styles offers opportunities to adapt to these differences. These communication strategies can be modified as the patient’s abilities and needs evolve during their ICU stay.
What Are Some Approaches That Can Enhance Communication in Pediatric Patients?
For children and adolescents who are navigating the ICU environment, it is critical for them to establish and develop trust in their health care team. Team members can approach pediatric patients with open and engaged attitudes that respect the patient’s boundaries and needs.33 Providers can begin each encounter by introducing themselves and telling the patient why they are there. By speaking directly to the patient and not limiting their attention to caregivers, providers can make the patient the focus of the conversation. While pediatric patients are intubated and receiving mechanical ventilation, they may benefit from using transitional objects (eg, blankets, stuffed animals, or fidget toys). Regardless of their developmental stage, children and adolescents should be encouraged to express their needs, convey their responses to critical illness, and participate in their care, thereby facilitating autonomy and control.33
Implementing strategies to enhance communication with critically ill children and adolescents improves their level of participation and the quality of care provided. Communication boards may present pictures of basic needs (eg, pain, fear, trouble sleeping), facilitating autonomy and self-expression as patients navigate communication barriers.34 Visual stimuli can be adapted to the patient’s educational level, featuring a combination of numbers, letters, and pictures. When developing and implementing communication strategies, proactive collaboration with speech-language therapists, child-life specialists, and family members optimizes opportunities for patients to express their needs. Once strategies are identified, signs at the patient’s bedside can be used to ensure that the approach is utilized by all team members. Frequent reassessment of the patient’s communication abilities and documenting effective communication strategies in the medical record and an ICU diary offer an approach to communicating with intubated pediatric patients.35
What Approaches Can Enhance Communication With Family, Friends, and Medical Teams?
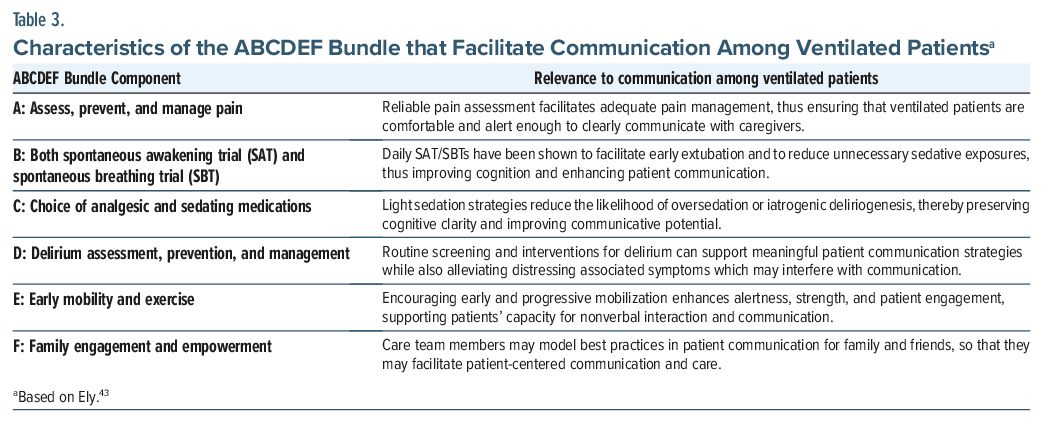
Family and friends can accelerate a loved one’s recovery from a critical illness through the implementation of simple strategies to optimize patient engagement and communication. They may be apprehensive to approach the bedside given the patient’s circumstances; however, with guidance and education about AAC and NVC strategies, they can serve as a voice for their loved ones, facilitating the patient’s expression of needs or concerns. Friends and family can also support the patient’s recovery by having an increased physical presence at the bedside, improving patient comfort using familiar items or music. They may bring in photographs of loved ones to brighten their hospital room and enhance their cognitive stimulation; moreover, displaying photographs can improve caregiver attitudes toward patients.36 Similarly, patients may enjoy listening to familiar music, which can also reduce heart rate and blood pressure.37 Friends and family may also find value in using evidence-based strategies to improve their loved ones’ recovery (eg, creating an ICU diary or using a “get to know me” style communication board).35,38 ICU diaries have reduced the development of mood and anxiety disorders and demonstrated numerous benefits for family members, serving as a tool to manage information, improve communication with the primary team, and enhance family coping.39,40 Families and clinicians have responded positively to initiatives such as the “get to know me” board,38,41 by humanizing patients, fostering communication between families and teams, and facilitating the team’s understanding of the patient’s values and wishes. The ICU Liberation Bundle, commonly referred to as the ABCDEF (or A–F) Bundle (see Table 3), emphasizes the value of family engagement as supported by numerous studies demonstrating improved patient outcomes when family presence is prioritized in the ICU.42,43
Members of the health care team can also greatly benefit from the same educational strategies and may be receptive to the implementation of additional teaching or didactic sessions to know when to incorporate different tools or approaches in the care of mechanically ventilated or otherwise nonverbal patients. Enhanced education for members of the health care team can facilitate downstream education of friends and family, thus prioritizing a culture that prioritizes patient self-expression and humanization.
Case Vignette Update
The psychiatric consultation team recommended the addition of a nondeliriogenic as-needed medication to manage breakthrough symptoms of anxiety and insomnia. They also advocated for the use of analgesics and sedatives with symptom-triggered analgesic boluses to target pain, thereby avoiding unnecessarily up-titration of Ms A’s basal rates of opioids or sedatives via continuous infusions. Ms A’s family participated eagerly in creating a “get to know me” board that highlighted her preferred name, music, and home hobbies and brought in photographs of family members and her pet dog. Ms A became more engaged and was able to remain calm during her SAT and spontaneous breathing trial on the following day, enabling her to be extubated successfully. However, after she was extubated, she continued to be anxious and afraid regarding the perceived mistreatment she felt had occurred earlier in her admission, although she no longer expressed concerns that she felt unsafe. She spent another 2 days in the ICU to maximize stabilization prior to transferring to an acute care floor, although she did not require readmission to the ICU during her hospitalization.
CONCLUSION
Communication difficulties associated with critical illness and mechanical ventilation increase the likelihood of developing neuropsychiatric sequelae of critical illness and can worsen short-and long-term patient outcomes. Nonetheless, ICU staff typically receive little training about how to communicate with intubated patients. The use of AAC and NVC strategies can enhance patient self-expression and facilitate meaningful communication among the patient, members of the health care team, and the patient’s friends and family. ICUs with limited resources may utilize “no-and low-technology” approaches, which include strategies to optimize patient communication, understanding, and comfort using simple writing tools or picture boards. “High-technology AAC tools,” such as keyboards, eye-tracking software, and VOCAs, can also enhance patient communication and care. Special populations including those with a tracheostomy, individuals with baseline intellectual or communication impairment, and those with limited English proficiency, and children, require the use of additional strategies and devices. As the culture of ICUs continues to evolve to prioritize lighter sedation strategies, patient communication becomes a natural target for improvement, enabling critically ill individuals to play an active role in their own care, appropriately restoring the individual to the center of their care and recovery.
Article Information
Published Online: July 2, 2026. https://doi.org/10.4088/PCC.25f04104
© 2026 Physicians Postgraduate Press, Inc.
Submitted: October 9, 2025; accepted March 10, 2026.
To Cite: Bui MP, Dietrich EA, Braford MB, et al. Communicating with intubated patients: challenges faced by health care providers, patients, and family members. Prim Care Companion CNS Disord 2026;28(4):25f04104.
Author Affiliations: Department of Psychiatry, Virginia Commonwealth University, Richmond, Virginia (Bui); Critical Care Psychiatry Service, Virginia Commonwealth University Health System, Richmond, Virginia (Bui); Department of Psychiatry and Neurobehavioral Sciences, University of Virginia, Charlottesville, Virginia (Dietrich); Consultation-Liaison Psychiatry Service, University of Virginia Medical Center, Charlottesville, Virginia (Dietrich); Lewis Gale Medical Center, Salem, Virginia (Braford, Mastronardi); Department of Psychiatry, Harvard Medical School, Boston, Massachusetts (Stern); Massachusetts General Hospital, Boston, Massachusetts (Stern).
Bui, Dietrich, Braford, and Mastronardi are co-first authors; Stern is the senior author.
Corresponding Author: Melissa P. Bui, MD, Department of Psychiatry, Virginia Commonwealth University, Richmond, Virginia ([email protected]).
Financial Disclosure: Dr Stern has received royalties from Elsevier for editing textbooks on Psychiatry. Drs Bui, Dietrich, Braford, and Mastronardi report no financial relationships.
Funding/Support: None.
Clinical Points
- Strategies that enhance communication among patients, health care providers, and family members reduce time spent on the ventilator and shorten hospital length of stay.
- Communication boards, with symbols and images, allow patients to point to them to indicate their needs.
- When attempting to read the lips of an intubated patient, health care providers should start with simple words and phrases and ask the patient to confirm that they are understanding what the patient has attempted to express.
- Since fluctuations in patients’ cognitive (due to delirium), psychological (eg, due to agitation, depression, and anxiety), and physical status may limit engagement with communication devices, it is helpful to employ a multifaceted approach.
References (43)

- Ashkenazy S, Weissman C, DeKeyser Ganz F. Perception of discomfort by mechanical ventilation patients in the intensive care unit: a qualitative study. Intensive Crit Care Nurs. 2021;64:103016. CrossRef
- Dithole K, Sibanda S, Moleki MM, et al. Exploring communication challenges between nurses and mechanically ventilated patients in the intensive care unit: a structured review. Worldviews Evidence-Based Nurs. 2016;13(3):197–206. CrossRef
- Perelló-Campaner C, González-Trujillo A, Alorda-Terrassa C, et al. Determinants of communication failure in intubated critically ill patients: a qualitative phenomenological study from the perspective of critical care nurses. Healthc (Basel). 2023;11(19):2645. CrossRef
- The Voice Foundation. The Voice Foundation: Advancing Understanding Of The Voice Through Interdisciplinary Research & Education. The Voice Foundation; 2013. https://voicefoundation.org/health-science/voice-disorders/anatomy-physiology-of-voice-production/. Accessed June 20, 2025
- Terragni P, Faggiano C, Martin EL, et al. Tracheostomy in mechanical ventilation. Semin Respir Crit Care Med. 2014;35(4):482–491.
- Ahmed RA, Boyer TJ. Endotracheal tube. 2023 Jul 24. In: StatPearls [Internet]. Treasure Island (FL). StatPearls Publishing; 2025. PMID: 30969569.
- Nomali M, Ayati A, Yadegari M, et al. Physical restraint and associated factors in adult patients in intensive care units: a cross-sectional study in North of Iran. Indian J Crit Care Med. 2022;26(2):192–198. CrossRef
- Karlsen MM, Holm A, Kvande ME, et al. Communication with mechanically ventilated patients in intensive care units: a concept analysis. J Adv Nurs. 2023;79(2):563–580.
- Zaga CJ, Berney S, Vogel AP. The feasibility, utility, and safety of communication interventions with mechanically ventilated intensive care unit patients: a systematic review. Am J Speech - Lang Pathol (Online). 2019;28(3):1335–1355. CrossRef
- Tate JA, Devito Dabbs A, Hoffman LA, et al. Anxiety and agitation in mechanically ventilated patients. Qual Health Res. 2012;22(2):157–173.
- Alkhateeb T, Semler MW, Girard TD, et al. Comparison of SAT and SBT conduct during the ABC trial and PILOT trial. J Intensive Care Med. 2025;40(1):3–9.
- Holm A, Dreyer P. Use of communication tools for mechanically ventilated patients in the intensive care unit. CIN. 2018;36(8):398–405.
- Yoshino Y, Unoki T, Sakuramoto H, et al. Association between intensive care unit delirium and delusional memory after critical care in mechanically ventilated patients. Nurs Open. 2021;8(3):1436–1443. CrossRef
- Jones C, Griffiths RD, Humphris G, et al. Memory, delusions, and the development of acute posttraumatic stress disorder-related symptoms after intensive care. Crit Care Med. 2001;29(3):573–580.
- Barry MJ, Edgman-Levitan S. Shared decision making-pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–781.
- Karmakar M, Panduragan S, Said F. Communication methods used with conscious intubated patients: scoping review. Open Nurs J. 2024;18:e18744346349706.
- Ten Hoorns S, Elbers PW, Girbes AR, et al. Communicating with conscious and mechanically ventilated critically ill patients: a systematic review. Crit Care. 2016;20(333):333.
- Elsahar Y, Hu S, Bouazza-Marouf K, et al. Augmentative and alternative communication (AAC) advances: a review of configurations for individuals with a speech disability. Sensors (Basel). 2019;19(8):1911.
- Al-Yahyai ANS, Arulappan J, Matua GA, et al. Communicating to non-speaking critically ill patients: augmentative and alternative communication technique as an essential strategy. SAGE Open Nurs. 2021;7:23779608211015234.
- Hall JA, Horgan TG, Murphy NA. Nonverbal communication. Ann Rev Psychol. 2019;70:271–294.
- Henricson M, Segesten K, Berglund AL, et al. Enjoying tactile touch and gaining hope when being cared for in intensive care—a phenomenological hermeneutical study. Intensive Crit Care Nurs. 2009;25(6):323–331.
- Rose L, Sutt AL, Amaral AC, et al. Interventions to enable communication for adult patients requiring an artificial airway with or without mechanical ventilator support. Cochrane Database Syst Rev. 2021;10(10):CD013379.
- Maringelli F, Brienza N, Scorrano F, et al. Gaze-controlled, computer-assisted communication in Intensive Care Unit: speaking through the eyes. Minerva Anestesiol. 2013;79(2):165–175.
- Ull C, Weckwerth C, Schildhauer TA, et al. First experiences of communication with mechanically ventilated patients in the intensive care unit using eye-tracking technology. Disabil Rehabilitation Assistive Technology. 2023;18(1):44–49. CrossRef
- Salem A, Ahmad MM. Communication with invasive mechanically ventilated patients and the use of alternative devices: Integrative review. J Res Nurs. 2018;23(7):614–630.
- Hess DR, Altobelli NP. Tracheostomy tubes. Respir Care. 2014;59(6):956–971. ; discussion 971-973.
- McRae J, Montgomery E, Garstang Z, et al. The role of speech and language therapists in the intensive care unit. J Intensive Care Soc. 2020;21(4):344–348.
- Freeman-Sanderson AL, Togher L, Elkins MR, et al. Return of voice for ventilated tracheostomy patients in ICU: a randomized controlled trial of early-targeted intervention. Crit Care Med. 2016;44(6):1075–1081.
- Mills CS, Michou E, King N, et al. Evidence for above cuff vocalization in patients with a tracheostomy: a systematic review. Laryngoscope. 2022;132(3):600–611.
- Pandian V, Boisen S, Mathews S, et al. Speech and safety in tracheostomy patients receiving mechanical ventilation: a systematic review. Am J Crit Care. 2019;28(6):441–450.
- Epstein SK. Anatomy and physiology of tracheostomy. Respir Care. 2005;50(4):476–482.
- Freeman-Sanderson A, Istanboulian L, Rose L. Communication with the critically ill patient: a nexus between patient needs, communication partner skills and the ICU environment. Intensive Crit Care Nurs. 2025;88:103962.
- Segers EW, Ketelaar M, de Man MACP, et al. How to support children to develop and express their coping preferences around minor invasive medical procedures: Children’s and parents’ perspectives. Eur J Pediatr. 2023;182(12):5553–5563. CrossRef
- Costello JM, Patak L, Pritchard J. Communication vulnerable patients in the pediatric ICU: Enhancing care through augmentative and alternative communication. J Pediatr Rehabil Med. 2010;3(4):289–301.
- Drumright K, Jones AC, Gervasio R, et al. Implementation of an intensive care unit diary program at a Veterans Affairs hospital. J Nurs Care Qual. 2021;36(2):155–161.
- Andersson M, Hall-Lord ML, Wilde-Larsson B, et al. Patient photographs—a landmark for the ICU staff: a descriptive study. Intensive Crit Care Nurs. 2013;29(4):193–201.
- Umbrello M, Sorrenti T, Mistraletti G, et al. Music therapy reduces stress and anxiety in critically ill patients: a systematic review of randomized clinical trials. Minerva Anestesiol. 2019;85(8):886–898. PubMed CrossRef
- Ahmad SR, Rhudy L, Barwise AK, et al. Perspectives of clinicians on the value of the get to know Me board in the ICU. Chest. 2025;167(2):561–570.
- McIlroy PA, King RS, Garrouste-Orgeas M, et al. The effect of ICU diaries on psychological outcomes and quality of life of survivors of critical illness and their relatives: a systematic review and meta-analysis. Crit Care Med. 2019;47(2):273–279. CrossRef
- Mickelson RS, Piras SE, Brown L, et al. The use and usefulness of ICU diaries to support family members of critically ill patients. J Crit Care. 2021;61:168–176. CrossRef
- Ahmad SR, Rhudy L, Fogelson LA, et al. Humanizing the intensive care unit: perspectives of patients and families on the Get to Know Me Board. J Patient Experience. 2023;10:23743735231201228. CrossRef
- Pun BT, Balas MC, Barnes-Daly MA, et al. Caring for critically ill patients with the ABCDEF Bundle: results of the ICU liberation collaborative in over 15,000 Adults. Crit Care Med. 2019 Jan;47(1):3–14. PubMed CrossRef
- Ely EW. The ABCDEF Bundle: science and philosophy of how ICU liberation serves patients and families. Crit Care Med. 2017;455(2):321–330.
Please sign in or purchase this PDF for $40.




