Abstract
Objective: Physicians inevitably face illness; yet, occupying the role of patient poses distinct psychological and professional challenges. To elucidate the unique challenges and strengths physicians may experience as patients, this study examines how popular media portrays physicians, highlighting common themes and their implications for clinical practice and medical education.
Methods: Literature was reviewed on the unique experiences of physicians in the role of patient. Searches were conducted on Google and ChatGPT using the terms movies + physician as patients, television + physician as patients, and popular media + physician as patients. Additional examples were drawn from the authors’ media knowledge base. Retrieved results were reviewed for depictions that exemplify the challenges and strengths unique to physician patients. Scenes from widely recognized films and television shows were discussed to illustrate key themes.
Results: Six recurring themes emerged: (1) shame and loss of professional identity, (2) interference in one’s own care through self-diagnosis, (3) fear of burdening colleagues, (4) difficulty relinquishing control, (5) curbside consultations with blurred boundaries, and (6) health literacy as a strength. These narratives reflect the physician health literature and offer resonant vignettes of the tensions physician patients face.
Conclusion: Physicians who become patients balance vulnerability with unique strengths, yet their professional identity often complicates care. Clinicians should anticipate these dynamics, set clear boundaries, and normalize help-seeking to ensure safe and dignified treatment. Media-based narratives can serve as powerful teaching tools, fostering empathy and preparing clinicians to navigate the complexities of caring for or assuming the role of physician patients.
Prim Care Companion CNS Disord 2026;28(3):26m04196
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Most people who have access to health care will at some point become a patient, whether during a routine checkup or an urgent trip to the operating room. Physicians are not exempt. While doctors experience unique challenges when they become patients, they also have unique strengths, stemming from their immersion and role in health care. Using popular media such as film and television is recognized as a useful tool to educate on complex psychosocial topics in medicine.1 To help readers understand the perspective of physicians when they inevitably become patients, we review the complexities of the physician patient’s experience and illustrate with examples from popular media that demonstrate various challenges the physician patient is likely to experience. These examples will allow readers the opportunity to recognize and understand the challenges that clinicians may face when treating physician patients. Furthermore, when doctors inevitably find themselves in the role of patient, it may prepare them to recognize, understand, avoid, and work through the situation more effectively.
When physicians are patients, the physician-patient alliance has both differences and similarities to that of the alliance with a nonphysician patient. Some of these differences may strain the doctor-patient relationship. Chief among the strengths is higher health literacy. However, this can be a double-edged sword since increased knowledge about the diagnosis or outcomes can lead to anxiety for the physician patient and difficulty coping.2 Various barriers to optimal health care in physicians have been discussed in the literature. One such impediment is embarrassment, including embarrassment when poor health stems from poor self-care. Mental health concerns may prove another such source of embarrassment that physicians do not wish to reveal to their colleagues. Furthermore, physicians may not want to impose on their colleagues by seeking medical care,3 or they may worry that seeking assistance with small concerns is an unwarranted use of resources. A culture of stoicism may make doctors uncomfortable with appearing vulnerable. This attitude, instilled during training, can continue throughout the lifetime of a physician.4 Difficulty relinquishing the role of the physician to the treating doctor may further complicate the physician patient’s health care relationships.5 Attempts to avoid the challenging aspects of the role of patient can lead to inappropriate curbside consultations when the ailing physician informally inquires with colleagues and friends rather than seeking care in the more typical setting of the office or the hospital. These curbside consultations may invite bias and inadequate history and examinations and so are more likely to result in faulty clinical conclusions. In addition, consulted physicians may find it difficult to share a poor prognosis with a peer.5 Together, these factors can result in suboptimal care, marked by strained communication, blurred roles, and uncertainty around how much control the physician patient should have in their own treatment.6
METHODS
An exploratory qualitative review of popular media was conducted to identify recurring portrayals of physicians who become patients. Searches were performed on Google and ChatGPT using the keywords movies + physician as patients, television + physician as patients, and popular media + physician as patients. The search aimed to capture well-known film and television shows and illustrative examples rather than a comprehensive dataset.
Media examples were screened for relevance based on 2 criteria: (1) the central character is a physician who assumes the patient role, and (2) the narrative depicts psychological or professional conflicts arising from this role shift. When multiple scenes addressed similar dynamics, those offering the clearest illustration of physician-patient challenges were selected.
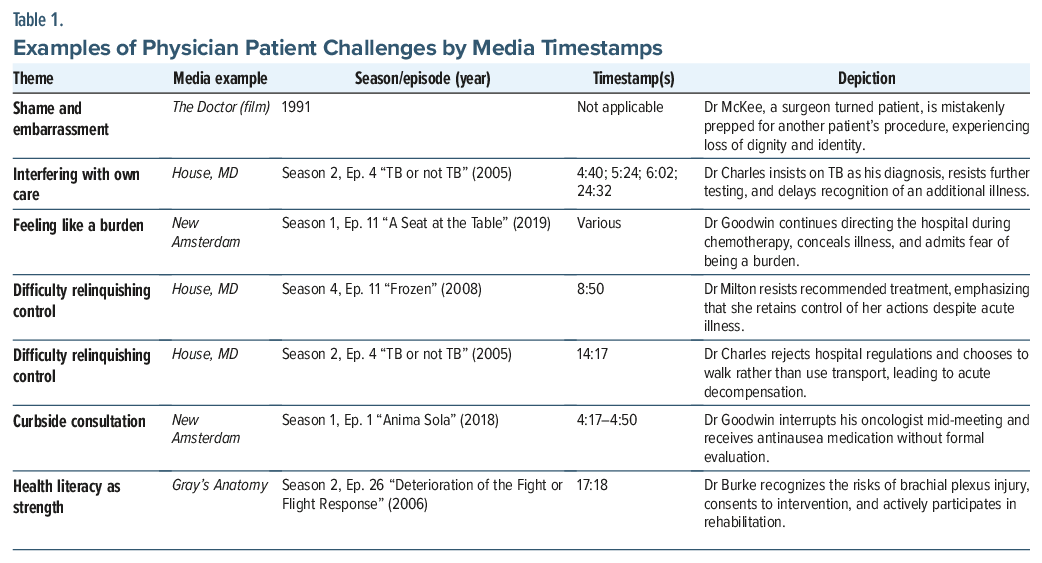
Six representative scenes from widely recognized works—The Doctor; House, MD; New Amsterdam; and Gray’s Anatomy—were chosen for thematic analysis. The authors independently reviewed and discussed each scene to identify key themes. Through consensus and informed by prior literature on the topic as reviewed above, 6 key themes were distilled: shame and embarrassment, interference in one’s own care, difficulty relinquishing control, fear of burdening colleagues, reliance on curbside consultations, and health literacy as a strength. Each theme is described with examples from film and television that illustrate how physicians experience unique aspects of the physician patient role.
RESULTS
Shame and Embarrassment
When a physician becomes a patient, the loss of professional identity can bring quiet but intense shame. In The Doctor (1991), Dr Jack McKee is a successful, emotionally detached surgeon who finds himself on the other side of the hospital bed after being diagnosed with throat cancer. During his workup, there is a moment when he is mistakenly prepped for a barium enema meant for someone else. He is groggy, dressed in a thin hospital gown, and wheeled into the wrong procedure without being asked or recognized. He does not speak up, not because he lacks authority but because he is stunned. This is not a power struggle. It is an emotionally raw moment of embarrassment, where he realizes he is no longer “Dr McKee.” He is just another patient in the system. The scene captures a deeply human subtlety: how shame can creep in, not from lack of control, but from being stripped of dignity in a setting that once defined his identity. It is a reminder that even the most experienced physicians are not immune to the emotional weight of vulnerability.
Interfering With Their Own Care
When a physician becomes a patient, the physician patient’s knowledge may lead them to interfere with their own care. They may offer their own differential, request unnecessary tests, deny necessary care, or use their wide breadth of knowledge to become part of their health care team in a deleterious fashion.2 A prime example of this is in House, MD, a show portraying the titular protagonist solving complicated medical mysteries, typically with awkward interpersonal interactions. In season 2, episode 4, “TB or not TB,” Dr Sebastian Charles helps treat tuberculosis in Africa. However, he himself becomes ill, necessitating a hospitalization at the hospital in which he works. During his hospital stay, he takes it upon himself to join Dr House’s team of physicians in their personal conference room. Dr House says, “Patients usually aren’t part of the diagnostic process,” to which Dr Charles replies, “Well, I’m a doctor,” while remaining in the consult room (4:40). He explains, “I’d like to stay and hear the differential” (5:24). Throughout the episode, he proclaims that he has tuberculosis even though his treatment team thinks otherwise. He resists tests and rejects anything that disagrees with his self-diagnosis. He remarks, “I don’t have time for this. It’s TB” (6:2). Dr Charles refuses any further testing since he is so convinced about his own diagnosis (24:32). In the end, it is found that, although he does have tuberculosis, he also has an insulinoma. Due to his focus on tuberculosis, which stems from his own expertise in infectious disease, Dr Charles inadvertently impedes his own care due to his failure to consider other causes. Ultimately, this negatively affects his care by delaying a definitive diagnosis and treatment.
Feeling Like a Burden
Physicians who become patients often worry about burdening their colleagues, loved ones, or care teams, which is a challenge frequently noted in narrative literature. This may stem from and/or engender a sense of guilt and perceived uselessness. Physician patients may feel uncomfortable accepting help, not because they doubt the clinical plan but because they believe their presence or need places an unfair strain on their colleagues or loved ones. This is portrayed in New Amsterdam, season 1, episode 11, “A Seat at the Table,” in which Dr Max Goodwin, the hospital’s medical director, begins chemotherapy while still trying to run the hospital. Rather than rest, he walks the halls with his intravenous pole, refusing to show any outward signs of illness. He pushes through exhaustion and nausea, avoiding any breaks and brushing off concerns from colleagues. When finally confronted, Dr Goodwin admits that he does not want to be treated differently or pitied, confessing his fear of becoming a burden to those who rely on him. His reluctance to lean on others is not rooted in pride or denial, but in a sense of duty, a belief that his illness might inconvenience or weaken those around him. This example illustrates how the internalized responsibility to always be the helper can prevent physician patients from receiving the care and compassion they themselves routinely give, ultimately delaying healing and emotional processing.
Difficulty Relinquishing Control
Just as feelings of burden can prevent physicians from accepting care, the discomfort of relinquishing control often leads them to interfere with their own treatment. It can be difficult for doctors to let go of the control that they are accustomed to having as the treatment provider.7 While relinquishing control of a difficult situation can be hard for anyone, this may be particularly difficult for doctors in the role of patient because this unfamiliar position challenges the physician’s previously established sense of identity. As a result, doctors may resist the role of the patient and interfere with their own care, not out of a problematic application of their own knowledge but out of the discomfort that comes from being a passenger in a difficult situation rather than being in the driver’s seat or from the wound that this might render to the doctor’s ego. This can be seen in House, MD, season 4, episode 11, “Frozen,” where a psychiatrist, Dr Milton, is acutely ill while stationed at an Antarctic base. In her discussion with Dr House, suggestions are made that Dr Milton agrees would be helpful, but she resists the recommendation due to her own ideological framework. She states, “You do realize only one of us has any control over my actions” (8:50). As the only physician at her base, she does not want to be treated as a patient and maintain her position as the doctor. In the episode “TB or not TB” of House, MD, the patient, Dr Charles, is being wheeled to get a pacemaker placed and chooses to take the stairs instead of the elevator. He remarks “I know, I know, hospital regulations” (14:17) in a dismissive fashion and then takes the stairs instead, which leads to his acute decompensation. In these examples, the patient is trying to hold onto the control that they had when they were physicians, ultimately negatively affecting their care.
Curbside Consult
Another way physicians attempt to preserve their autonomy while avoiding the patient role is through curbside consultations. This occurs when physicians informally seek medical advice from colleagues outside of the traditional physician-patient relationship. An example of this is in New Amsterdam. In the episode “Anima Sola,” season 1, episode 1, the protagonist Dr Goodwin ends up developing oropharyngeal cancer. While receiving chemotherapy, he experiences severe nausea and vomiting. He barges into the office of his oncologist, a colleague of his, and asks for help while she is in the middle of an international meeting. She cuts off the meeting and tells him “I’m happy to help. And you need anti-nausea meds.” (4:17–4:50) without doing any physical exam. In the end, this turns out to be the right choice for Dr Goodwin, but it easily could have gone badly. The oncologist assumed that it must have been his cancer and chemotherapy causing his symptoms, but no formal evaluation or exam was done before she determined the proper treatment. She let her personal biases for her colleague get ahead of her professional responsibilities as a physician and offered medical advice outside of the proper setting. Though it may be convenient for physicians to take this approach, it should be heavily cautioned against. This scene shows how professional familiarity can blur boundaries and lower the threshold for advice-giving. In real practice, such shortcuts risk misdiagnosis, since they bypass structured examinations.
Health Literacy as a Strength
In both literature and media, the vast knowledge that physicians carry is presented as not only a burden but also a strength. Doctors are more likely to understand their prognosis and be proactive in their own care.8 A prime example can be found in Gray’s Anatomy, season 2, episode 26, “Deterioration of the Fight or Flight Response.” In this episode, Dr Burke, a surgeon, is shot in his shoulder outside the hospital at which he works. The bullet is lodged in his brachial plexus, and with this knowledge, he knows that his arm and hand function are at risk. At first, he is reluctant to get a procedure done, but as his hand’s weakness and numbness worsens, he agrees to undergo it. During his discussion with the surgeon, he remarks “I could lose function of the entire arm” (17:18) and understands the gravity of the situation. After the operation, he is seen giving himself constant physical therapy by squeezing soft balls and other techniques to aid the recovery process. Dr Burke displayed excellent understanding of his diagnosis and prognosis and then took further action to increase his chances of making a full recovery. His medical training works to his advantage by motivating him to work on his own recovery but also enabling trust in his coworkers through shared and well-informed decision-making. Table 1 provides examples of physician patient challenges by timestamp.
DISCUSSION
When physicians become patients, they enter a psychologically complex and uncomfortable space that challenges their sense of identity, autonomy, and control. While their medical knowledge can be a source of strength that enables informed decision-making and proactive care, it can also lead to overreach, denial, or avoidance of formal treatment structures. Media portrayals offer a useful window into these tensions, capturing the internal conflict and interpersonal strain experienced by physician patients. Having spent their careers in the pursuit of helping others, physicians themselves deserve the opportunity to be cared for and supported in moments of illness. By understanding the barriers that we face as doctors and experiencing them through popular media, perhaps we can be prepared in advance to recognize, avoid, or address these barriers when they do present, both in physician patients and ourselves when we, ultimately, need medical care. Being forewarned in this way has the potential to both maintain dignity in a vulnerable time and to heal those who have healed so many others.
Article Information
Published Online: June 11, 2026. https://doi.org/10.4088/PCC.26m04196
© 2026 Physicians Postgraduate Press, Inc.
Submitted: November 24, 2025; accepted February 2, 2026.
To Cite: Pei M, Zhang V, Tyree E, et al. The patient in the mirror: understanding the role of doctor as patient through media. Prim Care Companion CNS Disord. 2026;28(3):26m04196.
Author Affiliations: Department of Psychiatry, Rutgers New Jersey Medical School, Newark, New Jersey (all authors).
Corresponding Author: Mingzhuo Pei, BA, Department of Psychiatry, Rutgers New Jersey Medical School, 185 South Orange Avenue, Newark, NJ 07103 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Clinical Points
- Physicians who become patients balance vulnerability with unique strengths, yet their professional identity often complicates care.
- Media-based narratives can serve as powerful teaching tools, fostering empathy and preparing clinicians to navigate the complexities of caring for or assuming the role of physician patients.
References (8)

- Kadivar M, Mafinejad MK, Bazzaz JT, et al. Cinemedicine: using movies to improve students’ understanding of psychosocial aspects of medicine. Ann Med Surg (Lond). 2018;28:23–27. PubMed CrossRef
- Tuttle JP. The physician’s disease: the impact of medical knowledge on personal illness. Palliat Support Care. 2007;5(1):71–76. PubMed CrossRef
- Kay M, Mitchell G, Clavarino A, et al. Doctors as patients: a systematic review of doctors’ health access and the barriers they experience. Br J Gen Pract. 2008;58(552):501–508. PubMed CrossRef
- Shadbolt NE. Attitudes to healthcare and self-care among junior medical officers: a preliminary report. Med J Aust. 2002;177(S1):S19–S20. PubMed
- Ende J, Kazis L, Moskowitz MA. Preferences for autonomy when patients are physicians. J Gen Intern Med. 1990;5(6):506–509. PubMed CrossRef
- Pullen D, Lonie CE, Lyle DM, et al. Medical care of doctors. Med J Aust. 1995;162(9):481–484. PubMed CrossRef
- Castro-Frenzel K. Physician-as-patient—vulnerabilities and strengths. JAMA. 2022;328(23):2303–2304. PubMed CrossRef
- Couser GP, Hagen PT, Swift MD, et al. Physician health series part one: characteristics of physicians as patients. Mayo Clin Proc. 2024;99(5):836–843. PubMed CrossRef
Please sign in or purchase this PDF for $40.




