Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2026;28(3):25f04172
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Have you wondered whether acute psychotic symptoms (eg, hallucinations and delusions) and thoughts of suicide are the only psychiatric sequelae of using psychedelics? Have you been unsure about which conditions might predispose someone to develop adverse psychological sequelae of psychedelic use? Have you heard that psychotic experiences may reemerge months after use of psychedelics? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Mr A, a 27-year-old man with mild asthma and chronic social anxiety, was brought to the emergency department (ED) by his brother roughly 4 hours after he developed intense perceptual changes and escalating paranoia following the ingestion of psilocybin mushrooms for the first time. On arrival at the ED, Mr A’s airway was intact, his oxygen saturation was normal, and his glucose level was within the normal range. He was oriented only to person and was markedly anxious, tremulous, and sensitive to sounds. Mr A was cooperative but restless, and he was frightened by an observer seen through the window. He was neither aggressive nor suicidal.
His medical workup was notable for stable vital signs, and his metabolic panel was unremarkable. Neuroimaging was deferred given Mr A’s absence of focal deficits or an altered consciousness. Urine toxicology only revealed the presence of cannabis (which he reported that he had smoked); he denied use of stimulants or serotonergic medications.
What Behavioral or Psychological Reactions Can Occur During and After a Psychedelic Experience?
While research is increasingly supporting the use of psychedelics for the treatment of psychiatric disorders and the promotion of well-being,1 adverse behavioral or psychological reactions can arise during and after psychedelic experiences (eg, transient perceptual changes, heightened emotional lability, troubling traumatic memories, changes in one’s sense of self, impaired cognition).2–4 While some of these experiences may be desired, benign, and promote healing in therapeutic contexts, they can also provoke intense fear, emotional distress, paranoia, confusion, or the fear of losing control, particularly in uncontrolled or unsupervised settings.2–4 Some individuals experience intense dysphoria, agitation, and restlessness or attempt to escape from their situation when they become distressed or disorientated. In rare cases, acute reactions lead to impulsive and unsafe behaviors in recreational contexts, when high doses of psychedelics are taken, when polysubstance use is involved, or when preexisting vulnerabilities (eg, a personal history of psychosis or a personality disorder) are present.2–4 Given the increasing prevalence of ED visits related to psychedelic use, health care providers should be cognizant of the acute and longer-term behavioral effects of psychedelics.5
After the acute effects of psychedelic use have subsided, some individuals may have persistent problems with emotional regulation, emotional destabilization, and derealization. Others report lingering anxiety, depression, or intrusive recollections that resemble trauma-related phenomena, particularly after an initial and intense experience.6 Even in the context of psychedelic-assisted therapy (PAT), new or worsening thoughts of suicide have been reported in clinical trials7 and after recreational use.8 Although persistent adverse effects (AEs) (eg, prolonged psychosis, exacerbation of underlying psychiatric conditions, triggering of manic episodes, or maladaptive behavioral changes) are uncommon in controlled clinical settings, they have been documented in unsupervised settings; these sequelae have largely been attributed to predisposing psychiatric conditions.9 Hallucinogen persisting perception disorder (HPPD) is a rare AE in which an individual may experience lasting or persistent visual hallucinations or perceptual distortions after using psychedelic substances, alongside distress or impairment in functioning.10 Although the etiology of this condition is unknown, it may be of heterogeneous origin, with some cases more related to underlying psychological predisposition and others related to neurobiological changes. HPPD has not been observed in modern clinical trials of psychedelics.11
How Does a History of Trauma Influence the Risks and Outcomes of Psychedelic Experiences?
The role of trauma in impacting the postpsychedelic clinical course has come under increasing scrutiny in recent years. Although research on classic psychedelics as well as entactogens for the treatment of posttraumatic stress disorder continues to expand,12 growing evidence also suggests that individuals with a history of trauma may require more support and additional therapy sessions and present unique risks such as worsening of traumatic symptoms following psychedelic sessions.13,14 One recent study examining naturalistic psychedelic use found that individuals with a history of adverse childhood experiences (ACEs) were more likely to report psychological difficulties following psychedelic use, with increasing ACE burden conferring greater risk.15
In addition, the possibility of experiencing recovered memories—whether accurate or not—has also been documented in early-phase research in the middle of the 20th century, as well as in some present-day studies.16,17 Given that a common aspect of psychedelic states is the intensely felt reality of whatever is being experienced, how to approach the patient who believes they recovered previously unknown traumatic memories during psychedelic experiences remains unclear and a point of controversy in the field.17,18 While a full exploration of this question is beyond the scope of this article, it is important that patients are aware that these experiences can and do occur, including in therapeutic settings, and that patients with a known history of trauma may face unique risks with respect to psychedelic exposure.
What Factors Predispose Individuals to Adverse Reactions?
While clinical research on PAT is promising, AEs with serious consequences can occur (eg, involving the emergence or worsening of psychiatric symptoms). Research into the mechanisms of the therapeutic efficacy of psychedelics has offered clues to understanding this risk. One widely referenced model, known as the relaxed beliefs under psychedelics model, posits that serotonergic psychedelics “decrease the precision weighting of neurobiologically encoded beliefs.”19 While this model proposes how psychedelics can catalyze change, it may also explain why psychological destabilization arises under the influence of psychedelics (eg, questioning beliefs that once helped a person make sense of their world can jeopardize ego defenses and leave individuals psychologically vulnerable without proper support).
Emerging research has identified certain factors that may influence the risk of various forms of psychological destabilization from PAT. Appropriate screening of eligible patients is perhaps the most effective way to reduce this risk; many research protocols exclude participants with a personal or family history of bipolar disorder or psychotic-spectrum illnesses, as this population is at higher risk of adverse psychological events during PAT. However, more recent data suggest that PAT may be beneficial in some forms of bipolar disorder.20 In addition, neuroticism is associated with a higher likelihood of adverse psychological events following psychedelic use.21 While screening based on personality traits is not recommended, awareness of traits that influence the risk of adverse psychological events in PAT can inform how therapists approach treatment protocols.
Using a protocol that involves preparation and integration is integral in minimizing the risk of adverse psychological reactions, as community reports of prolonged AEs frequently involve situations that lack professional guidance.22 A key component of PAT is the challenging nature of the psychedelic experience; some research has found a positive correlation between problematic experiences and enduring increases in well-being.23 Acknowledging this, preparation and integration create the scaffolding that allows patients to derive benefit from potentially challenging psychedelic experiences, with preparation serving to create the therapeutic relationship necessary to support challenging experiences, and integration serving to help individuals create meaning that can catalyze psychological change.24 As such, when appropriate, the number of preparation and integration sessions offered can be increased to ensure a patient’s comfort and safety. Recent qualitative research corroborates this, finding that patients with “serious mood, anxiety, or trauma-related disorders” may need different amounts of preparation and integration.25 Additionally, research suggests that the degree of trust developed during the preparatory phase can influence the efficacy of treatment; moreover, a lack of preparation can lead to feeling overwhelmed and having difficulty navigating the psychedelic experience, which can lead to a greater risk of AEs.26
How Should Clinicians Manage Agitation or Psychosis Following Psychedelic Use?
Agitation that develops during an acute psychedelic experience is best managed by use of nonpharmacologic and de-escalatory strategies (that emphasize reassurance, environmental calming, and a steady therapeutic presence). Moreover, harm-reduction frameworks highlight the importance of maintaining a nonjudgmental stance, using simple orienting cues and reflective language, reducing sensory stimulation, and prioritizing safety without resorting to coercive measures, unless they are absolutely necessary.24,27 Evidence suggests that this supportive, grounded approach can substantially reduce psychedelic-related distress, which helps individuals regain a sense of safety and allows for the resolution of agitation without medical interventions or risking harm to themselves or others.9,27 Harm-reduction work balances the principles of autonomy, cultural humility, and noncoercive care, even within acute care settings, where safety is often a priority.24,27,28
If nonpharmacologic strategies fail to resolve behavioral issues and an individual poses a risk to themselves or others, judicious use of benzodiazepines (eg, lorazepam) should be considered as a first-line treatment for acute anxiety, panic, or behavioral dysregulation in EDs. Antipsychotics should be avoided, in general, during the initial phase of intoxication, unless symptoms are severe, persistent, or incompatible with psychedelic effects. For persistent psychotic symptoms that fail to resolve on their own, a comprehensive psychiatric assessment and use of second-generation antipsychotics (SGAs) are usually recommended,29 given that 5-hydroxytryptamine 2A receptor (5-HT2A) blockade with SGAs has been shown to produce more complete antagonism of psychedelic effects, whereas first-generation antipsychotics, such as haloperidol, may worsen psychotic-like effects.30 After stabilization, referral for integrative psychotherapy or community supports may aid in processing of the experience, reduce recurrence of distress, and connect individuals to ongoing mental health care, when needed.27
How Can Persistent Psychoses or Severe Behavioral Disturbances Be Managed?
When agitation evolves into frank psychosis—characterized by sustained hallucinations, delusional thinking, or severe disorganization beyond the expected time course of psychedelic intoxication—timely psychiatric evaluation is warranted. Clinicians should assess for precipitating factors (eg, an underlying mood or psychotic disorder, polysubstance use, sleep deprivation, or medical contributors, such as metabolic disturbances). For persistent or severe symptoms, antipsychotic medication is appropriate, with atypical antipsychotic agents typically preferred due to their favorable side effect profiles. Hospitalization may be required for diagnostic clarification, stabilization, or safety monitoring. Postpsychedelic use episode follow-up is essential, as individuals who develop persistent psychosis may be predisposed to psychotic or bipolar disorders. Integration-focused psychotherapy, psychoeducation, and harm-reduction counseling support recovery and help mitigate recurrence. Across settings, clinicians should approach agitation and psychosis associated with use of psychedelics with a trauma-informed, nonstigmatizing framework that balances patient autonomy with safety.
Can Perceptual Disturbances From One Psychedelic Be Distinguished From Another?
Although different psychedelics have been associated with characteristic phenomenological features, it is important to emphasize that clinicians cannot reliably identify which psychedelic substance has been used based on phenomenology alone. The subjective effects of psychedelics overlap substantially across compounds and are strongly influenced by dose, route of administration, and contextual factors such as set and setting. As a result, phenomenological descriptions are best understood as broadly informative rather than diagnostically definitive in clinical settings.
Psychedelics are serotonin receptor agonists, a property that helps explain their ability to induce perceptual disturbances, particularly visual alterations such as geometric patterns and kaleidoscopic imagery. These agents also heighten the perception of music, sounds, and bodily sensations; sensory input, such as music, can in turn influence the qualitative features of the visual experience.31
Psychedelic experiences share broad similarities across different psychedelic substances. All psychedelics cause altered visual, auditory and sensory perception, synesthesia, changes in emotion and cognition, ego dissolution, and mystical experiences. However, subtle differences abound. In fact, some older literature refers to psychedelics as “hallucinogens,” although “psychedelic” is the preferred term today. It is important to note that, in contrast to delirium and some psychoses, psychedelics produce perceptual alterations and illusions rather than true hallucinations, where individuals experience drug-induced perceptual disturbances as being real.32 This can help to distinguish the effects of psychedelics from other hallucinatory states, such as psychosis, delirium, and the effects of psychotogenic drugs, such as cocaine and methamphetamine, where the experiences are often perceived as genuine.
Tryptamine psychedelics, such as psilocybin and lysergic acid diethylamide (LSD), are the most studied psychedelics. LSD has been thought to have more intense visual experience and cognitive disintegration, although both drugs can induce similar experiences that may be indistinguishable to clinicians. Nonetheless, they differ in their duration of the effects. The effects of psilocybin last about 4–6 hours, whereas those of LSD can last between 8 and 15 hours.33 In addition, subtle phenomenological differences have been observed. For instance, Holze et al34 compared the perceptual disturbances of psilocybin and LSD in 28 healthy participants and found that LSD had longer-lasting and earlier-onset effects than those of psilocybin; however, they were otherwise phenomenologically indistinguishable. Moreover, participants who received LSD showed more cognitive disorganization and more complex imagery and had audiovisual synesthesia. The authors also noted that users of LSD were more prone to the altered meaning of percepts.4 N, N-dimethyltryptamine (DMT) is a tryptamine psychedelic with a very short duration of effect when taken parenterally or inhaled (ie, 5–20 minutes). In contrast to other classic psychedelic drugs, DMT frequently produces rapid, intense, and vivid visual hallucinations characterized by changing geometric patterns and a felt sense of being in a different world.35 The experience or visualization of insect-or reptile-like entities is common.35,36 DMT is not orally bioavailable due to rapid metabolism by monoamine oxidase; however, it is a component of ayahuasca, a decoction containing both plant-derived DMT and monoamine oxidase–inhibiting compounds. In this form, which is taken orally, the effects are prolonged for up to 8 hours.37
Phenethylamine psychedelics, such as mescaline (contained in peyote and San Pedro), have been described as being more empathogenic and less hallucinatory. The phenylethylamine (2,5-dimethoxy-4-bromophenethylamine [2C-B]) is a psychedelic with a molecular structure similar to mescaline. Both mescaline and 2C-B induce similar perceptual changes (eg, euphoria, empathy, and physical sensations, such as a warm bodily feeling and tingling). Mystical experiences and ego dissolution are less pronounced with phenethylamine entheogens. However, the duration of the experience varies, with 2C-B lasting approximately 4–6 hours, while mescaline’s effects persist for 10–14 hours.38 When Mallaroni and colleagues39 analyzed the phenomenological differences between 2C-B, psilocybin, and placebo in 20 healthy participants, they found similar perceptual disturbances; however, the subjective effects abated more quickly after the use of 2C-B as compared to psilocybin. Users of 2C-B and psilocybin each experienced visual alterations, an altered perception of time, and cognitive and emotional changes. However, the depth of the experience was less intense with 2C-B as compared to psilocybin. Participants who received psilocybin experienced heightened affect and an alteration of the self. Instead, 2C-B induced elation, like a similarly acting entactogen.39 Concurrent use of LSD and 3,4-methylenedioxymethamphetamine (MDMA) is prevalent in recreational settings, particularly within dance music scenes. This combination, commonly referred to as “candy flipping,” is reported by users to enhance positive and empathogenic effects; however, a controlled laboratory study found no substantial differences in peak subjective effects between LSD alone and the combined administration of LSD and MDMA.40 This discrepancy may reflect expectancy effects, contextual factors, or methodological features of the study, including fixed dosing, simultaneous administration, and the use of a highly controlled clinical setting, which may limit the detection of more subtle or time-dependent experiential differences.
Lastly, the phenomenology of ketamine is highly variable but prominently features perceptual changes (auditory, visual, and proprioceptive); detachment from body, self, emotions, and the world; and experiences of stillness or spaciousness.41 While it is frequently referred to as a “dissociative” drug, this term has been criticized as failing to capture the range of effects this drug may produce.42
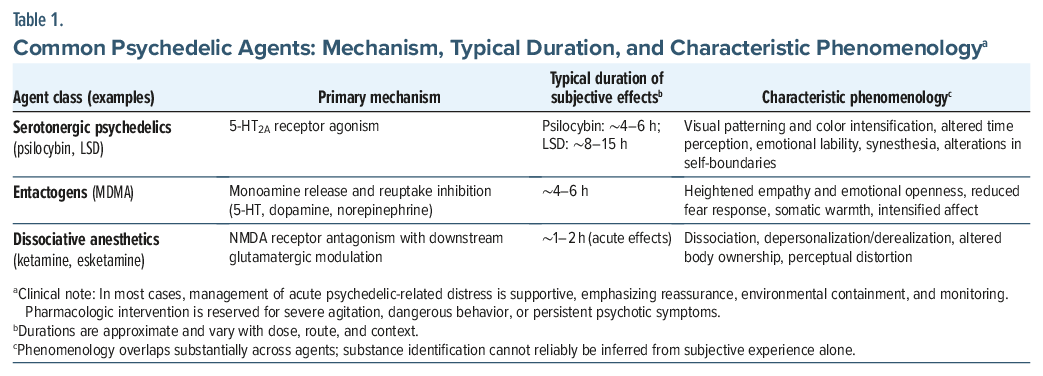
Understanding the phenomenology of psychedelics and their duration of effects can help psychiatrists, ED physicians, and toxicologists recognize and evaluate risk profiles. Since all psychedelics can induce similar perceptual disturbances, as well as changes in mood and cognition changes, it can be difficult to distinguish which drug has been used, by relying upon the onset, intensity, and duration of the experience. Clinicians should familiarize themselves with the phenomenology of different tryptamine and phenethylamine psychedelics to differentiate their effects from those of other conditions, such as drug intoxication, mania, psychotic disorders, and delirium. Table 1 provides a summary of the phenomenological characteristics of commonly used classes of psychedelics.
Why Do Some Individuals Develop Persistent Psychosis or Perceptual Disturbances After Use of Psychedelics?
Persistent psychosis or enduring perceptual disturbances following psychedelic use appear to be uncommon, particularly in controlled or clinical settings; however, when they do occur, they raise important questions about vulnerability, context, and risk stratification. The diversity of settings, doses, and patterns of psychedelic use complicates the assessment of long-term psychological and psychiatric risks, as the effects of these drugs are exquisitely sensitive to contextual and interpersonal factors. Moreover, our understanding of these risks and risk factors remains incomplete, as most modern clinical trials of psychedelics involve small sample sizes and highly selective inclusion and exclusion criteria. Common exclusions include suicide risk, substance use disorders, and personal or family histories of psychosis or bipolar disorder; as a result, these samples do not reliably generalize to the broader population.
For this reason, much of the current understanding of risk factors for prolonged adverse reactions to psychedelics derives either from naturalistic use or from the published literature from the first wave of psychedelic research in the 1950s and 1960s. This earlier research contains a substantial body of data, given that as many as 40,000 individuals were administered psychedelic drugs in experimental or clinical settings, compared with approximately 2,000 individuals dosed across all clinical trials in the entire 21st century.25,43 The fact that both research and clinical practice operated under far less stringent guidelines during this earlier era may increase the utility of these reports, insofar as psychedelics were frequently administered to patients who would be ineligible by modern clinical trial standards, such as patients with schizophrenia.
Early psychedelic research with LSD explicitly distinguished between risks in healthy volunteers and those treated for clinical conditions, with the latter viewed as requiring more intensive supervision and monitoring.16 This distinction is less clearly articulated in much of the modern clinical literature, which predominantly studies psychiatric populations under highly controlled conditions. Suggestibility, expectancy, and enthusiasm for psychedelics were also historically identified as risk factors for prolonged reactions.16,44 Case reports described prolonged psychosis or recurrence of perceptual disturbances following LSD use in individuals with a history of schizophrenia,45 although more recent naturalistic evidence suggests that this association may be less definitive than previously assumed.46 Repeated exposure to psychedelic drugs has also been reported in case series of individuals presenting with postpsychedelic persistent hallucinosis.47
Contemporary evidence remains mixed. While case reports document prolonged psychosis following exposure to psychedelic drugs, this has often been clouded by the presence of comorbid cannabis use, which is itself an established risk factor for the development of psychosis.48 More broadly, coingestants and chronic substance use patterns complicate causal attribution in naturalistic settings and should be considered when adverse outcomes are attributed to psychedelic exposure. Population-based cohort studies, including genetically informative twin studies, as well as survey data, have not identified a clear association between psychedelic use and worsened psychotic symptoms in individuals with risk factors for, or a personal history of, psychotic disorders.49,50 In contrast, some evidence suggests an association with increased psychotic symptoms among individuals with risk factors for bipolar disorder.51
HPPD remains understudied. Survey data suggest associations between premorbid sensory hyperreactivity and the development of HPPD, with affected individuals reporting higher rates of sensory conditions such as eye floaters, photosensitivity and phonosensitivity, tinnitus, migraine with aura, vertigo, and paresthesias.11,52 Premorbid anxiety may also predispose toward the development of HPPD.11 However, a recent large survey of naturalistic psychedelic drug users found no difference in neuroticism scores between individuals reporting the presence or absence of HPPD.53 That same study identified a history of mental health symptoms and use of nonpsychedelic substances as correlating with a higher likelihood of psychologically distressing HPPD. Identifying risk factors for the development of prolonged psychosis and perceptual disturbance remains a critical unmet need, particularly as interest in psychedelic use continues to expand both within and outside of clinical settings.
Are There Absolute Contraindications to Use of Psychedelics, and What Are the Potential Benefits of Use?
Universally accepted absolute contraindications to psychedelic use are lacking. In practice, however, most contemporary protocols exclude adolescents and those with psychotic disorders, bipolar I disorder, or significant medical comorbidities. These exclusions reflect a precautionary approach grounded in limited and context-dependent safety data rather than definitive evidence of harm.
Consistent with concerns outlined above, contemporary clinical trials have generally excluded individuals with psychotic disorders or bipolar I disorder.28 Yet, emerging meta-analytic data suggest that these risks may be more modest and context-dependent than once believed. Although available data suggest that the incidence of psychedelic-induced psychosis is low— including a 3.8% rate in uncontrolled schizophrenia samples and a 0.6% incidence across randomized controlled trials—these findings have nonetheless prompted debate about whether schizophrenia should remain a categorical exclusion.46
Serious AEs (eg, worsening depression, suicidal behavior, psychosis, or convulsive episodes) occur in roughly 4% of participants who have preexisting neuropsychiatric conditions.2 Of note, neither suicide nor persistent psychosis or HPPD has been reported in modern supervised settings following high-dose sessions. In addition, catastrophic outcomes in recreational contexts have not been observed within structured research environments.2
The risk of unmasking bipolar disorder, particularly through treatment-emergent mania, remains a prominent concern. Bipolar disorder is frequently misdiagnosed as unipolar depression, and the consequences of a missed diagnosis can be profound.54 Small pilot studies in bipolar II depression have shown encouraging signals of safety and efficacy, with large positive effect sizes and no observed episodes of hypomanic or manic switches or an increase in suicide attempts55; however, no trials have included individuals with bipolar I disorder, and case reports continue to document manic activation under less controlled circumstances,54 highlighting the need for cautious selection of participants.
Drug-drug interactions represent another important consideration in psychedelic use (medical and physiological interactions are reviewed in greater detail in a companion article in the PCC).56 Concurrent monoamine oxidase inhibitor (MAOI) use is considered an absolute contraindication due to the risk of serotonin syndrome, particularly with ayahuasca and related combinations of DMT and an MAOI.57 Although this risk would not theoretically apply to simple 5-HT2A agonists such as psilocybin, cases of hypertensive emergency have been reported when psilocybin mushrooms—but not synthetic psilocybin—were combined with MAOIs.58,59
In contrast, selective serotonin reuptake inhibitors (SSRIs) occupy a more ambiguous clinical position. While some studies suggest attenuation of subjective psychedelic effects, others demonstrate preserved antidepressant efficacy. Escitalopram pretreatment has not been shown to diminish positive mood effects of psychedelics compared to placebo,60 and 1 open-label study reported substantial reductions in depressive symptoms with psilocybin therapy among individuals on chronic SSRI treatment.61 However, SSRI tapering—sometimes required by study protocols—carries its own risks, including mood destabilization. While further evidence is needed as to whether SSRIs attenuate therapeutic effects of classic psychedelics, current consensus is that they are safe when combined with SSRIs.
Survey-based evidence has suggested an increased risk of seizures when classical psychedelics are combined with lithium,62 although a recent study of psilocybin in individuals with bipolar II disorder did not require discontinuation of mood stabilizers; instead, lithium doses were held the night before dosing sessions.63 Significant knowledge gaps persist. No published clinical trials that investigated the use of classical psychedelics in adolescents have been completed, although 4 trials (of psilocybin and MDMA) have been registered.64 Whether older adults may face unique psychiatric risks from classical psychedelics, or require dosing adjustments for altered pharmacokinetics, is also unknown, as few older adults are included in contemporary clinical trials.65 It is likewise unclear whether the presence of neurocognitive disorder may confer an unacceptable risk; however, research is currently proposed to study these conditions with psychedelics given the potential for their neuroplasticity-enhancing effects to restore or repair functional connectivity in areas of the brain impacted by neurodegeneration.66 Lastly, while ketamine has been shown to be safe in older adults with depression, it may be less effective than in younger patients.67
In light of these uncertainties, a conservative, case-by-case approach remains prudent. Careful screening for personal or family histories of psychotic and bipolar disorders, clarification of prior manic symptoms, assessment of concurrent substance use, and review of potential drug-drug interactions are central to risk mitigation (medical contraindications and physiological risks are addressed in a companion review).56 Individuals with diagnostic uncertainty, complex psychopharmacologic regimens, or elevated genetic or clinical vulnerability to mania warrant heightened caution and closer monitoring. When administered in supervised clinical settings, structured preparation, conservative dosing, and postsession follow-up appear to substantially reduce serious adverse outcomes; however, important knowledge gaps persist for adolescents, older adults, and individuals with neurocognitive disorders. As the evidence base expands, some historical exclusions may narrow, but for practicing hospital clinicians, the landscape remains best characterized as promise tempered by substantial uncertainty.
What Happened to Mr A?
Mr A was managed with supportive de-escalation within a low-stimulus environment. He received lorazepam 1 mg, which reduced his restlessness within 20 minutes. He was reassured that his symptoms were expected effects of a time-limited intoxication and that there is no evidence of a new medical illness. Over the next hour, his paranoia diminished, and his terror evaporated; he became self-conscious and embarrassed. No manifestations of mania or depression developed.
Within 10 hours of his psychedelic ingestion, he was fully oriented, affectively regulated, and free from persistent perceptual distortions or safety concerns. He was observed in the ED for 2 additional hours; given that symptoms did not recur, he was discharged to home with his brother with a referral for community integration-focused counseling and guidance on mitigating anxiety in the future. His presentation resolved within a timeframe that was consistent with usual acute psilocybin intoxications.
CONCLUSIONS
Psychological complications from psychedelics, although rare in clinical settings, can emerge unpredictably and may take varied forms, from transient anxiety to more persistent disturbances. While evidence suggests that these compounds hold significant therapeutic potential, especially in carefully controlled settings, ongoing research must continue to address the full spectrum of possible adverse outcomes. Significant knowledge gaps exist regarding risks in special populations (eg, patients with psychotic disorders, bipolar disorders, or a history of trauma, as well as young adults and geriatric individuals). Clinicians should remain aware of these risks, particularly in vulnerable populations, and approach psychedelic use without stigma but with judicious caution.
Article Information
Published Online: June 25, 2026. https://doi.org/10.4088/PCC.25f04172
© 2026 Physicians Postgraduate Press, Inc.
Submitted: December 18, 2025; accepted May 27, 2026.
To Cite: King F, Zambrano J, Mauney E, et al. Psychological adverse effects of psychedelic use. Prim Care Companion CNS Disord 2026;28(3):25f04172.
Author Affiliations: Center for Neuroscience of Psychedelics, Massachusetts General Hospital, Boston, Massachusetts (King); Department of Psychiatry, Harvard Medical School, Boston, Massachusetts (King, Zambrano, Nigam, Espi Forcen, Taylor, Mattson, Stern); Department of Psychiatry, Massachusetts General/McLean Hospital, Boston, Massachusetts (Zambrano, Nigam, Mattson, Stern); Center for Neurointestinal Health, Department of Gastroenterology, Massachusetts General Hospital, Boston, Massachusetts (Mauney); Division of Pediatric Gastroenterology, Hepatology, and Nutrition, Tufts Medical Center, Boston, Massachusetts (Mauney); Lincoln Residence Program, McLean Hospital, Boston, Massachusetts (Espi Forcen); Cleveland Clinic Psychiatric Treatment Resistance Program, Cleveland Clinic, Cleveland, Ohio (Barnett); Home Base Massachusetts General Hospital, Boston, Massachusetts (Taylor); Neurotherapeutics Department, McLean Hospital, Boston, Massachusetts (Taylor).
King, Zambrano, Mauney, Nigam, and Espi Forcen are co-first authors; Stern is the senior author.
Corresponding Author: Franklin King IV, MD, Department of Psychiatry, Harvard Medical School, Boston, Massachusetts ([email protected]).
Financial Disclosure: Dr King serves on the Scientific Advisory Board of Apex Labs; has previously held personal stock in Compass Pathways and Cybin; and has received research support from Tryp Therapeutics, the David Borsook Project, and the Tiny Blue Dot Foundation. Dr Mauney has received research support from Tryp Therapeutics. Dr Barnett holds stock in Atai Life Sciences N.V. and CB Therapeutics (options); has served as an advisor for AbbVie, CB Therapeutics, Compass Pathways, GH Research, LivaNova, Janssen, and MindMed; and receives monetary compensation for editorial work from DynaMed Plus (EBSCO Industries, Inc), speaker’s fees from TD Cowen, and research support from Abbott Laboratories, Compass Pathways, MindMed, and Reunion Neuroscience. Dr Stern has received royalties from Elsevier for editing textbooks on psychiatry. Drs Zambrano, Nigam, Espi Forcen, Taylor, and Mattson have no disclosures to report.
Funding/Support: None.
Clinical Points
- Although rare and absent in modern clinical trials, hallucinogen persisting perception disorder (HPPD) can cause lasting visual disturbances and functional impairment; clinicians should be aware that individuals with premorbid sensory sensitivity, anxiety, or complex psychiatric histories may be at elevated risk for HPPD.
- Initial management of psychedelic-related agitation should prioritize noncoercive, calming strategies; benzodiazepines may be used if safety is a concern, while antipsychotics should be reserved for severe or persistent symptoms.
- It remains unclear whether psychedelics truly pose a significant risk of causing psychotic disorders. Among individuals with existing psychotic disorders, population-level data suggest that the risk may be lower than once assumed, although case reports of harm exist. These patients are typically excluded from trials, making it difficult to draw firm conclusions.
References (67)

- Cavarra M, Falzone A, Ramaekers JG, et al. Psychedelic-assisted psychotherapya systematic review of associated psychological interventions. Front Psychol. 2022;13:887255. CrossRef
- Hinkle JT, Graziosi M, Nayak SM, et al. Adverse events in studies of classic psychedelics: a systematic review and meta-analysis. JAMA Psychiatry. 2024;81(12):1225–1235. CrossRef
- Kopra EI, Ferris JA, Rucker JJ, et al. Adverse experiences resulting in emergency medical treatment seeking following the use of lysergic acid diethylamide (LSD). J Psychopharmacol. 2022;36(8):956–964. CrossRef
- Simonsson O, Goldberg SB, Chambers R, et al. Psychedelic use and psychiatric risks. Psychopharmacol Berl. 2025;242(7):1577–1583. CrossRef
- Garel N, Tate S, Nash K, et al. Trends in hallucinogen-associated emergency department visits and hospitalizations in California, USA, from 2016 to 2022. Addiction. 2024;119(5):960–964. CrossRef
- Perna J, Trop J, Palitsky R, et al. Prolonged adverse effects from repeated psilocybin use in an underground psychedelic therapy training program: a case report. BMC Psychiatry. 2025;25(1):184. CrossRef
- Meshkat S, Malik T, Zeifman R, et al. Psychedelics and suicide-related outcomes: a systematic review. J Clin Med. 2025;14(5):1416. CrossRef
- Jones G, Arias D, Nock M. Associations between MDMA/ecstasy, classic psychedelics, and suicidal thoughts and behaviors in a sample of U.S. adolescents. Sci Rep. 2022;12(1):21927. CrossRef
- Day JK, Grooff MTH. Freedom of recreation: a critique of the prohibition, decriminalization, and legal regulation of psychedelics for recreational use. Contemp Drug Probl. 2025:00914509251371749.
- Doyle MA, Ling S, Lui LMW, et al. Hallucinogen persisting perceptual disorder: a scoping review covering frequency, risk factors, prevention, and treatment. Expert Opin Drug Saf. 2022;21(6):733–743. CrossRef
- Halpern JH, Lerner AG, Passie T. A review of hallucinogen persisting perception disorder (HPPD) and an exploratory study of subjects claiming symptoms of HPPD. Curr Top Behav Neurosci. 2016;36:333–360.
- Mitchell JM, Mo G, Kolk Bvan der, et al. MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial. Nat Med. 2023;29(10):2473–2480. CrossRef
- Simon G, Tadmor N, Skragge M, et al. Recalled childhood trauma and post-psychedelic trajectories of change in a mixed-methods study. Sci Rep. 2025;15(1):42852. CrossRef
- Bender DA, Nayak SM, Siegel JS, et al. Provider perspectives on challenges in treatment during psychedelic therapy. Psychopharmacology. 2025:1–8. Published online. CrossRef
- Olofsson M, Osika W, Goldberg SB, et al. Difficulties following naturalistic psychedelic use and associations with adverse childhood experiences. Int J Drug Polic. 2026;148:105105. CrossRef
- Cohen S. Lysergic acid diethylamide: side effects and complications. J Nerv Ment Dis. 1960;130(1):30–40. PubMed CrossRef
- Peck SK, Brewerton TD, Fisher H, et al. Therapeutic emergence of dissociated traumatic memories during psilocybin treatment for anorexia nervosa. J Eat Disord. 2025;13(1):89. CrossRef
- Kangaslampi S, Wolff M, Doss MK, et al. Questioning the recovery of dissociated traumatic memories under psilocybin: comment on “Therapeutic emergence of dissociated traumatic memories during psilocybin treatment for anorexia nervosa.”. J Eat Disord. 2025;13(1):278. CrossRef
- Zeifman RJ, Spriggs MJ, Kettner H, et al. From relaxed beliefs under psychedelics (REBUS) to revised beliefs after psychedelics (REBAS). Sci Rep. 2025;15(1):3651. CrossRef
- Gard DE, Pleet MM, Bradley ER, et al. Evaluating the risk of psilocybin for the treatment of bipolar depression: a review of the research literature and published case studies. J Affect Disord Rep. 2021;6:100240. CrossRef
- Barrett FS, Johnson MW, Griffiths RR. Neuroticism is associated with challenging experiences with psilocybin mushrooms. Pers Individ Differ. 2017;117:155–160. PubMed CrossRef
- Evans J, Robinson OC, Argyri EK, et al. Extended difficulties following the use of psychedelic drugs: a mixed methods study. PLOS ONE. 2023;18(10):e0293349. CrossRef
- Carbonaro TM, Bradstreet MP, Barrett FS, et al. Survey study of challenging experiences after ingesting psilocybin mushrooms: acute and enduring positive and negative consequences. J Psychopharmacol. 2016;30(12):1268–1278. PubMed CrossRef
- Gorman I, Nielson EM, Molinar A, et al. Psychedelic harm reduction and integration: a transtheoretical model for clinical practice. Front Psychol. 2021;12:645246. CrossRef
- Bender DA, Nayak SM, Siegel JS, et al. Psychological support approaches in psychedelic therapy. J Clin Psychiatry. 2025;86(1). CrossRef
- Breeksema JJ, Niemeijer A, Kuin B, et al. Holding on or letting go? Patient experiences of control, context, and care in oral esketamine treatment for treatment-resistant depression: a qualitative study. Front Psychiatry. 2022;13:948115. CrossRef
- Pleet MM, White J, Zamaria JA, et al. Reducing the harms of nonclinical psychedelics use through a peer-support telephone helpline. Psychedelic Med New Rochelle. 2023;1(2):69–73. CrossRef
- Barber GS, Dike CC. Ethical and practical considerations for the use of psychedelics in psychiatry. Psychiatr Serv. 2023;74(8):838–846. CrossRef
- Sulstarova A, Scheuerlein L, Monari S, et al. Treatment approaches and efficacy in psychedelic-induced psychosis: a systematic review. Asian J Psychiatry. 2025;110:104604. CrossRef
- Vollenweider FX, Vollenweider-Scherpenhuyzen MF, Bäbler A, et al. Psilocybin induces schizophrenia-like psychosis in humans via a serotonin-2 agonist action. Neuroreport. 1998;9(17):3897–3902. PubMed CrossRef
- Forcen FE. A psilocybin experience gone wrong: the importance of psychedelic assisted psychotherapy. J Psychoact Drugs. 2025:1–3. ahead-of-print(ahead-of-print).
- Garcia-Romeu A. Deconstructing the trip treatment: are hallucinogenic effects critical to the therapeutic benefits of psychedelics?. NPPDigit Psychiatry Neurosci. 2025;3(1):22. CrossRef
- Nutt D, Castle D, eds. Psychedelics as Psychiatric Medications. Oxford Psychiatry Library. Oxford University Press; 2023. Accessed December 17, 2025.
- Holze F, Ley L, Müller F, et al. Direct comparison of the acute effects of lysergic acid diethylamide and psilocybin in a double-blind placebo-controlled study in healthy subjects. Neuropsychopharmacology. 2022;47(6):1180–1187. CrossRef
- Lawrence DW, Carhart-Harris R, Griffiths R, et al. Phenomenology and content of the inhaled N, N-dimethyltryptamine (N, N-DMT) experience. Sci Rep. 2022;12(1):8562. CrossRef
- Luan LX, Eckernäs E, Ashton M, et al. Psychological and physiological effects of extended DMT. J Psychopharmacol. 2024;38(1):56–67. PubMed
- Ruffell S, Netzband N, Bird C, et al. The pharmacological interaction of compounds in ayahuasca: a systematic review. Braz J Psychiatry. 2020;42(6):646–656. PubMed CrossRef
- Papaseit E, Farré M, Pérez-Mañá C, et al. Acute pharmacological effects of 2C-B in humans: an observational study. Front Pharmacol. 2018;9:206. PubMed CrossRef
- Mallaroni P, Mason NL, Reckweg JT, et al. Assessment of the acute effects of 2C-B vs. psilocybin on subjective experience, mood, and cognition. Clin Pharmacol Ther. 2023;114(2):423–433. PubMed
- Straumann I, Ley L, Holze F, et al. Acute effects of MDMA and LSD co-administration in a double-blind placebo-controlled study in healthy participants. Neuropsychopharmacology. 2023;48(13):1840–1848. PubMed
- Breeksema JJ, Niemeijer A, Kuin B, et al. Phenomenology and therapeutic potential of patient experiences during oral esketamine treatment for treatment-resistant depression: an interpretative phenomenological study. Psychopharmacology. 2023;240(7):1547–1560. PubMed
- Schalkwyk GIvan, Wilkinson ST, Davidson L, et al. Acute psychoactive effects of intravenous ketamine during treatment of mood disorders: analysis of the Clinician Administered Dissociative State Scale. J Affect Disord. 2017;227:11–16. PubMed
- Grinspoon L, Bakalar JB. Psychedelic Drugs Reconsidered. Basic Books; 1979.
- McGlothlin W, Cohen S, McGlothlin MS. Long lasting effects of LSD on normals. Arch Gen Psychiatry. 1967;17(5):521–532. PubMed CrossRef
- Frosch WA, Robbins ES, Stern M. Untoward reactions to lysergic acid diethylamide (LSD) resulting in hospitalization. N Engl J Med. 1965;273(23):1235–1239. PubMed CrossRef
- Sabé M, Sulstarova A, Glangetas A, et al. Reconsidering evidence for psychedelic-induced psychosis: an overview of reviews, a systematic review, and meta-analysis of human studies. Mol Psychiatry. 2025;30(3):1223–1255. PubMed
- Rosenthal SH. Persistent Hallucinosis following repeated administration of hallucinogenic drugs. Am J Psychiatry. 1964;121(3):238–244. PubMed
- Morris SL. A case report of psilocybin-induced psychosis in a predisposed patient. Clin Psychopharmacol Neurosci. 2024;22(4):684–687. CrossRef
- Simonsson O, Mosing MA, Osika W, et al. Adolescent psychedelic use and psychotic or manic symptoms. JAMA Psychiatry. 2024;81(6):579–585. PubMed
- Dourron HM, Bradley M, Simonsson O, et al. Naturalistic psychedelic use and psychotic symptoms: a cross-sectional study of individuals with a personal or family history of psychotic or bipolar disorders. Psychedelic Med. 2025;3(2):93–102. CrossRef
- Honk L, Stenfors CUD, Goldberg SB, et al. Longitudinal associations between psychedelic use and psychotic symptoms in the United States and the United Kingdom. J Affect Disord. 2024;351:194–201. PubMed
- McConnell A, He W, McConnell H, et al. The never-ending trip: associations between hallucinogen persisting perception disorder (HPPD) and non-visual perceptual disturbances. J Psychedelic Stud. 2025;9(3):212–220. CrossRef
- Hadley M, Halliday A, Stone JM. Association of hallucinogen persisting perception disorder with trait neuroticism and mental health symptoms. J Psychoact Drugs. 2025;57(1):47–53. CrossRef
- Hosein MM, Reid MJ, Walser S, et al. Considerations and cautions for the integration of psilocybin into routine clinical care: a consensus statement from the US National Network of depression Centers’ Task Group on psychedelics and related compounds. eClinicalMedicine. 2025;89:103517. PubMed
- Do A, Cloutier L, Hébert-Tremblay L, et al. Psilocybin use in bipolar disorder: a comprehensive review. J Affect Disord. 2026;394(Pt B):120485. PubMed
- King F, Barnett BS, Taylor ST, et al. Medical complications of psychedelics. Prim Care Companion CNS Disord. 2026;28(3):25f04171.
- Malcolm B, Thomas K. Serotonin toxicity of serotonergic psychedelics. Psychopharmacology. 2022;239(6):1881–1891. PubMed
- Barnett BS, Koons CJ, Eynde VVden, et al. Hypertensive emergency secondary to combining psilocybin mushrooms, extended release dextroamphetamine-amphetamine, and tranylcypromine. J Psychoact Drugs. 2025;57(3):297–303.
- Vojtĕchovský M, Hort V, Safratová V. [Influence of MAO inhibitors on psilocybine induced psychosis]. Act Nerv Super. 1968;10(3):278–279. PubMed
- Becker AM, Holze F, Grandinetti T, et al. Acute effects of psilocybin after escitalopram or placebo pretreatment in a randomized, double-blind, placebo-controlled, crossover study in healthy subjects. Clin Pharmacol Ther. 2022;111(4):886–895. PubMed
- Goodwin GM, Croal M, Feifel D, et al. Psilocybin for treatment resistant depression in patients taking a concomitant SSRI medication. Neuropsychopharmacology. 2023;48(10):1492–1499. PubMed
- Nayak S, Gukasyan N, Barrett F, et al. Classic psychedelic coadministration with lithium, but not lamotrigine, is associated with seizures: an analysis of online psychedelic experience reports. Pharmacopsychiatry. 2021;54(05):240–245. PubMed
- Rosenblat JD, Meshkat S, Doyle Z, et al. Psilocybin-assisted psychotherapy for treatment resistant depression: a randomized clinical trial evaluating repeated doses of psilocybin. Med. 2024;5(3):190–200.e5. PubMed
- Rajwani K, Jacobs E, Bruce L, et al. Clinical psychedelic research in adolescents: a scoping review and overview of ethical considerations. Lancet Child Adolesc Heal. 2025;9(10):744–752. CrossRef
- Bouchet L, Sager Z, Yrondi A, et al. Older adults in psychedelic-assisted therapy trials: a systematic review. J Psychopharmacol. 2024;38(1):33–48. PubMed
- Winkelman MJ, Szabo A, Frecska E. The potential of psychedelics for the treatment of Alzheimer’s disease and related dementias. Eur Neuropsychopharmacol. 2023;76:3–16. PubMed
- Zheng W, Zhou YL, Wang CY, et al. A comparative analysis of antidepressant and anti-suicidal effects of repeated ketamine infusions in elderly and younger adults with depression. J Affect Disord. 2023;334:145–151. PubMed
Please sign in or purchase this PDF for $40.




