Abstract
Background: Medication nonadherence is a multifaceted challenge in psychiatric treatment, driven by clinical, psychosocial, and patient factors. An understudied aspect is the physical properties of solid oral dosage forms (SODFs)—shape, size, and color—which may influence acceptability and adherence. Yet, quantitative evidence connecting real-world preferences to adherence outcomes is scarce, especially in psychiatric settings.
Objective: To evaluate preferences for tablet shape, size, and color among psychiatric outpatients and their relation to self-reported adherence.
Methods: This cross-sectional observational study, conducted over 6 months (April–October 2024) in a tertiary psychiatric unit, included 232 patients with varied psychiatric diagnoses on oral medications. Sociodemographics, clinical details, and preferences/dislikes for tablet attributes (shape: flat circular vs oval/oblong; size: small, medium, large; color: white, yellow, red, blue) were gathered via a structured questionnaire. Adherence was measured using the validated 10-item Medication Adherence Rating Scale (score ≥6=adherent). Associations were analyzed with χ2 and Fisher exact tests (P<.05).
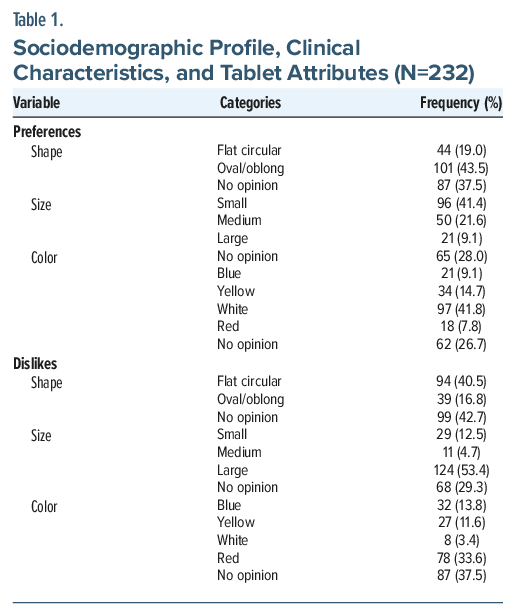
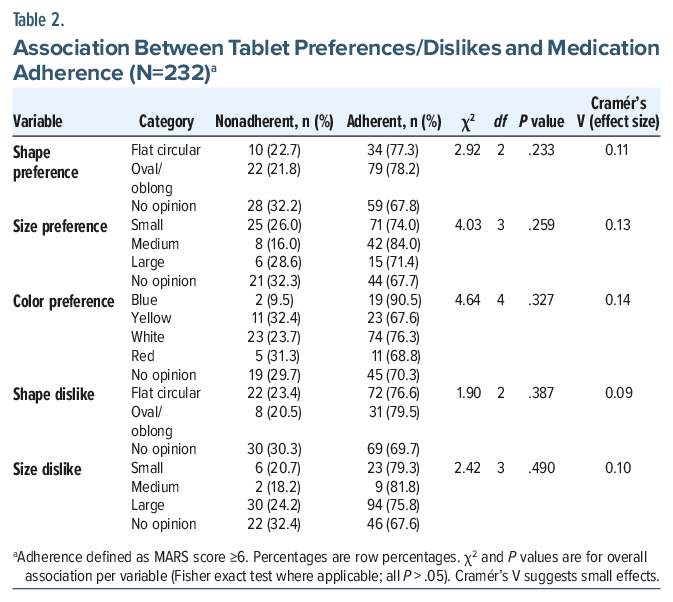
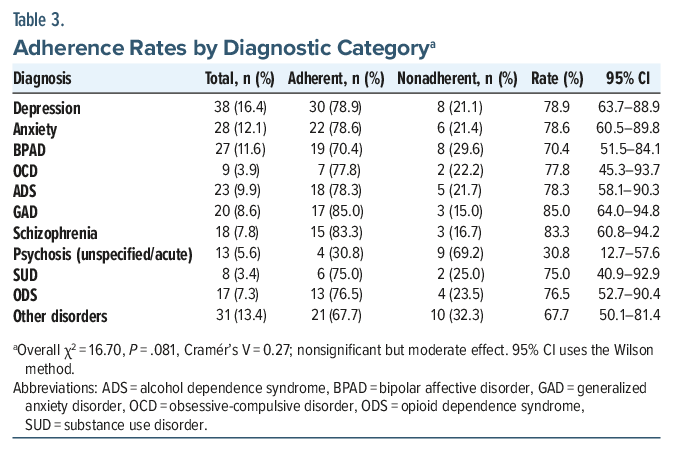
Results: The cohort (mean age: 36±13.3 years; 65.1% male) had 74.1% adherence (95% CI, 68.1–79.3%). Preferences included oval/oblong shapes (43.5%), small sizes (41.4%), and white colors (41.8%); dislikes were large sizes (53.4%), flat-circular shapes (40.5%), and red colors (33.6%). No significant links existed between preferences/dislikes and adherence (all P >.05; χ2 = 1.90–4.64; Cramér’s V=0.09–0.14). Adherence rates varied by diagnosis (lowest in psychosis: 30.8%; 95% CI, 12.7–57.6% and highest in generalized anxiety disorder: 85.0%; 95% CI, 64.0–94.8%) but nonsignificantly (χ2 =16.70, P= .081, Cramér’s V=0.27).
Conclusion: Psychiatric patients show distinct esthetic preferences for tablets, consistent with prior acceptability research, but these do not predict adherence. Clinical symptoms, illness insight, and therapeutic alliance appear to dominate. Strategies should emphasize psychosocial interventions rather than formulation esthetics.
Prim Care Companion CNS Disord 2026;28(4):25m04101
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Nonadherence to medication is one of the most widespread and severe issues in managing severe and persistent mental illnesses. The World Health Organization estimates that adherence to long-term therapies in developed countries averages 50%, often lower in psychiatric conditions—for instance, 40%–70% nonadherence in schizophrenia, decreasing to 26% among homeless individuals.1 Far from simple disobedience, nonadherence is multifaceted, driving poor outcomes such as treatment relapse, symptom exacerbation, rehospitalization, and increased mortality.2,3 This relapse cycle burdens health care systems, individuals, and society, with medical costs rising 23% due to extended stays and interventions.3,4 Thus, identifying and mitigating nonadherence factors remains a core priority in psychiatric care.4
Beyond well-documented clinical and psychosocial barriers, medication acceptability, encompassing the sensory experience of solid oral dosage forms (SODFs) including shape, size, color, taste, odor, and ease of swallowing, critically influences treatment continuity. These physical attributes initiate patient-drug interaction, evoking psychological and emotional responses that shape willingness to adhere, as supported by studies on SODF preferences.5,6
Adherence entails accurate use of prescribed drugs at correct doses, timing, and duration; however, psychiatric disorders such as schizophrenia, bipolar disorder, and major depression impose barriers via emotional dysregulation, cognitive deficits, and poor illness insight.3,7 Nonadherence manifests as intentional (eg, deliberate omission due to side effect fears or efficacy doubts) or unintentional (eg, forgetfulness, unclear instructions, or formulation issues).3,4 In psychiatry, both types stem from patient factors (eg, cognitive impairments), environmental elements, and systemic obstacles, with SODF design playing a pivotal role independent of pharmacologic effects.5–7 Psychiatric patients face heightened risks of readmission, relapse, and death from nonadherence, exacerbating economic strains in resource-limited settings.2,3 Addressing this demands multifaceted strategies, including psychoeducation and cognitive-behavioral interventions, alongside evaluating patient traits and drug design to enhance adherence rates.4,7 Despite the global recognition of these challenges, there remains a striking paucity of studies exploring the interplay between SODF attributes and adherence, specifically within the Indian subcontinent—a region characterized by diverse cultural beliefs, socioeconomic disparities, and high psychiatric morbidity rates. This gap is particularly critical, as localized insights are essential for tailoring interventions that account for region-specific barriers such as stigma, polypharmacy, and limited access to palatable formulations, underscoring the urgent need for contextually relevant research to bridge this void and improve outcomes in this vulnerable population.
METHODS
This cross-sectional observational study enrolled 232 adult outpatients (aged ≥18 years) with diverse psychiatric diagnoses (eg, depression, anxiety, bipolar affective disorder) who were taking oral medications for at least 1 month. Exclusion criteria included acute psychosis, cognitive impairment precluding informed consent, or inability to complete questionnaires. Participants were recruited consecutively over 6 months (April–October 2024) from the psychiatric outpatient department. The protocol of the study, consent forms, and all data collection tools were ethically approved by the Institutional Ethics Committee (Reference No. SGRR/IEC/24/24, dated October 28, 2024). Written informed consent was obtained from all participants. Data were collected via a structured questionnaire assessing sociodemographics (eg, age, gender, education), clinical characteristics (diagnosis, illness duration), and preferences/dislikes for tablet attributes (shape: flat circular vs oval/oblong; size: small, medium, large; color: white, yellow, red, blue) on a Likert-style scale (1=strongly prefer/dislike to 5=no opinion). Medication adherence was measured using the validated 10-item Medication Adherence Rating Scale (MARS), with scores ≥6 indicating adherence.8 Ethical consent was obtained from all participants, ensuring confidentiality. Statistical analysis was performed using jamovi (version 2.4).9 Descriptive statistics included means±SDs for continuous variables and frequencies (%) for categorical variables. Associations between preferences/dislikes and adherence were tested via χ2 tests and Fisher exact test (P<.05 significance). Effect sizes were calculated using Cramér’s V. Confidence intervals (95%) for proportions used the Wilson method. Subgroup analyses by diagnosis were conducted. The sample size designed for the study was 231, which was generated by the SCALEXSP software with the confidence interval at 95%, expected prevalence of 5.1%, and margin of error of ±3%, including patients of all genders.
RESULTS
The cohort comprised 232 patients (mean age: 36 ± 13.3 years, 65.1% male, 56.5% married). Common diagnoses included depression (16.4%), anxiety (12.1%), and bipolar affective disorder (11.6%), with a median illness duration of 36 months (SD = 48). Past/family medical history was absent in 94.4% and 95.7%, respectively. Overall adherence was 74.1% (MARS score: 6–10; 95% CI, 68.1–79.3%), with the lowest rate in psychosis (30.8%; 95% CI, 12.7–57.6%) and the highest in generalized anxiety disorder (85.0%; 95% CI, 64.0–94.8%; Table 3 provides subgroup details). Preferences favored oval/oblong shapes (43.5%), small sizes (41.4%), and white colors (41.8%). Dislikes centered on large sizes (53.4%), flat-circular shapes (40.5%), and red colors (33.6%) (Table 1). Clinical variables (eg, diagnosis [Supplementary Tables 1 and 2]) showed no impact on adherence (P = .081 to P = .760). No significant associations emerged between any preference/dislike and adherence (all P > .05; χ2 = 1.90–4.64; Cramér’s V = 0.09–0.14; Table 2).
DISCUSSION
Our findings reveal distinct patient preferences for tablet attributes—oval shapes, small sizes, and white colors—aligning with prior reports emphasizing ease of swallowing and neutral esthetics. For instance, a cross-sectional study found that white was the preferred color for tablets, attributing this preference to familiarity and reduced stigma perceptions.10 Similarly, experimental work on SODFs confirmed small, noncircular shapes as optimal for acceptability, particularly in polypharmacy scenarios common in psychiatry.5,6 Dislikes for large, red tablets echo concerns over dysphagia risks and negative emotional associations (eg, red evoking danger).6
Despite these preferences, no significant link to adherence emerged, suggesting that while organoleptic factors influence initial acceptability, they exert limited predictive power on sustained compliance in psychiatric outpatients. This finding contrasts with general medicine studies where shape/size preferences correlated with higher adherence rates10,11 but aligns with psychiatric-specific evidence, indicating dominance of clinical determinants such as symptom severity and therapeutic alliance.3,4,7 In our cohort, the lowest adherence in psychosis (30.8%) likely reflects insight deficits rather than formulation issues, underscoring that psychosocial barriers (eg, intentional nonadherence from side effect fears) overshadow esthetics.2,4 Psychosocial issues such as stigma and lack of social support, illness severity (eg, severe symptoms impairing judgment), therapeutic alliance (eg, poor trust reducing compliance by up to 50%), and contextual factors (eg, family dynamics in India) further modulate adherence, often more than physical attributes.14,15 These results advocate for integrated interventions: psychoeducation on formulations alongside cognitive-behavioral strategies to bolster adherence.3,4
This study relies on the self-reported MARS, which may overestimate adherence due to recall and social desirability biases; validation studies show only moderate concordance with objective measures (ĸ=0.4–0.6).8,12,13 We could not include objective adherence measures (eg, pill counts or medication event monitoring system) due to resource constraints in our outpatient setting. The cross-sectional design precludes causality inference, and the single-center urban cohort limits generalizability to rural or more diverse Indian populations, where socioeconomic and cultural factors may differ. Additionally, our analysis did not adjust for confounders via multivariable models, which future studies should explore. Future multicenter trials with objective measures (eg, pill counts) are warranted, especially in diverse Indian contexts.7
In conclusion, tablet esthetics matter for acceptability but not adherence in psychiatry. Prioritizing holistic care over formulation tweaks could optimize outcomes in this vulnerable population.
Article Information
Published Online: June 30, 2026. https://doi.org/10.4088/PCC.25m04101
© 2026 Physicians Postgraduate Press, Inc.
Submitted: October 4, 2025; accepted February 27, 2026.
To Cite: Rawat R, Thapliyal P, Kumar R, et al. Beyond pharmacology: do tablet shape, size, and color influence medication adherence in psychiatric outpatients? Prim Care Companion CNS Disord 2026;28(4):25m04101.
Author Affiliations: Department of Pharmacy Practice, School of Pharmaceutical Sciences, Shri Guru Ram Rai University, Dehradun, Uttarakhand, India (Rawat, Thapliyal, Kumar, Joshi); Department of Psychiatry, Shri Guru Ram Rai Institute of Medical and Health Sciences, Shri Guru Ram Rai University, Dehradun, Uttarakhand, India (Garg).
Corresponding Author: Shobit Garg, MD, DPM, Department of Psychiatry, Shri Guru Ram Rai Institute of Medical and Health Sciences, Shri Guru Ram Rai University, Dehradun, Uttarakhand 248001 India ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
ORCID: Yogesh Joshi: https://orcid.org/0000-0002-9105-923X; Shobit Garg: https://orcid.org/0000-0001-5913-9021
Supplementary Material: Available at Psychiatrist.com.
Clinical Points
- Psychiatric outpatients prefer small, oval/oblong, white tablets, but these preferences do not significantly predict adherence—prioritize addressing clinical symptoms and insight over esthetic changes.
- Adherence is notably lower in psychosis (30.8%) compared to other diagnoses such as generalized anxiety disorder (85.0%), highlighting the need for targeted psychoeducation and alliance building in insight-deficient groups.
- Holistic strategies, including cognitive-behavioral interventions and family involvement, should complement formulation design to overcome psychosocial barriers in resource-limited settings.
References (15)

- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. WHO; 2003.
- Melle I, Friis S, Haahr U, et al. Non-adherence to antipsychotic medication, relapse and rehospitalisation in recent-onset schizophrenia. BMC Psychiatry. 2008;8:32. PubMed
- Sendt KV, Tracy DK, Bhattacharyya S. A systematic review of factors influencing adherence to antipsychotic medication in schizophrenia-spectrum disorders. Psychiatry Res. 2015;225(1-2):14–30. PubMed
- Velligan DI, Weiden PJ, Sajatovic M, et al. The Expert Consensus Guideline Series: Adherence Problems in Patients With Serious and Persistent Mental Illness. J Clin Psychiatry. 2009;70(Suppl 4):1–46. PubMed
- Kurczewska-Michalak M, Lewek P, Matyjaszczyk M, et al. Patients’ preferences and willingness to Pay for solid forms of oral medications-results of the Discrete Choice experiment in polish outpatients. Int J Environ Res Public Health. 2020;17(5):1613. PubMed
- Overgaard ABA, Møllgaard B, Hansen CM, et al. Patients’ evaluation of shape, size and colour of solid dosage forms. Pharm World Sci. 2001;23(5):185–188. PubMed
- Ramamurthy P, Jayasree A, Solomon S, et al. Medication nonadherence and its associated factors in psychiatric patients in India: a systematic review and meta-analysis. Indian J Psychiatry. 2023;65(5):506–525. PubMed
- Fialko L, Garety PA, Kuipers E, et al. A large-scale validation study of the Medication Adherence Rating Scale (MARS). Schizophr Res. 2008;100(1-3):53–59. PubMed
- The Jamovi Project. Jamovi. Version 2.4. Sydney, Australia; 2023. Available from:. https://www.jamovi.org
- Wondmkun YT, Mulaw MD. Patients’ preference for Pharmaceutical dosage forms: Does it Affect medication adherence? A cross-sectional study in Community Pharmacies. Patient Prefer Adherence. 2024;18:753–766. PubMed
- Walsh JC, Mandigo TR, Williams RM, et al. Responses to a 1 month self-report on adherence to antiretroviral therapy are consistent with electronic data and virological treatment outcome. AIDS. 2002;16(2):269–277. PubMed
- Shi L, Liu J, Koleva Y, et al. Concordance of adherence measurement using self-reported adherence questionnaires and medication monitoring devices. Pharmacoeconomics. 2010;28(12):1097–1107.
- Witry M, Hoang H, Jacobs NA, et al. A systematic review of primary care-focused, self-reported medication adherence tools. J Am Pharm Assoc. 2023;63(2):477–490.e1.
- Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892–909. PubMed
- Grover S, Chakrabarti S, Sharma A, et al. Attitudes toward psychotropic medications among patients with chronic psychiatric disorders and their family caregivers. J Neurosci Rural Pract. 2014;5(4):374-383. PubMed
Please sign in or purchase this PDF for $40.




