Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2026;28(3):25f04171
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Have you ever wondered how prevalent and problematic medical complications of psychedelics are? Have you been uncertain about why adverse effects (AEs) arise and how they can be managed? Have you been ill-equipped to answer questions from your patients about the long-term sequelae of psychedelic use? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Mr B, a 23-year-old man with no significant medical history, was brought to the emergency department (ED) by paramedics after collapsing at an outdoor music festival. According to bystanders, Mr B had been dancing for several hours in hot weather before becoming disoriented, paranoid, and agitated. He reportedly ingested a tab of what he believed was lysergic acid diethylamide (LSD) earlier in the evening. During his transport to the ED, he had a brief tonic-clonic seizure. On arrival to the ED, he was confused (and unable to provide a history), combative, hyperthermic (core temperature 39.7°C [103.46°F]), hypertensive, diaphoretic, and tachycardic and had dilated pupils, generalized muscle rigidity, and visual hallucinations.
Laboratory testing revealed signs of rhabdomyolysis (eg, an elevated creatine kinase and myoglobinuria). His serum sodium level was low, and liver function tests were mildly elevated. Neuroimaging and a lumbar puncture were deferred given the absence of focal deficits and the clinical impression that he was suffering from a toxidrome. Urine toxicology was positive only for tetrahydrocannabinol.
DISCUSSION
How Common and Serious Are Acute Medical Complications of Psychedelic Use?
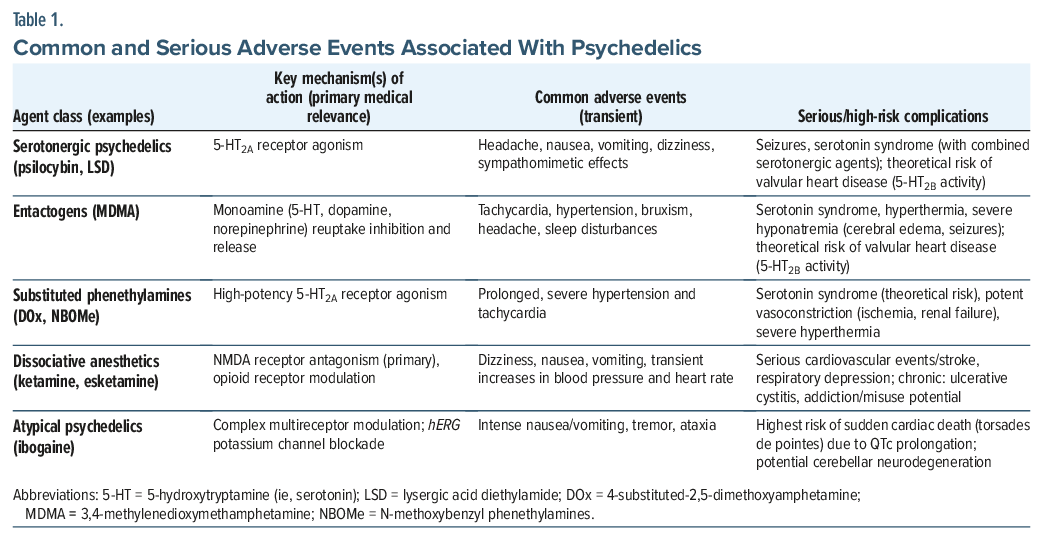
Although medical complications associated with psychedelic use are uncommon and typically brief in controlled clinical settings, serious AEs can occur, especially when used at high dosages and in those with underlying medical and psychiatric conditions (Table 1). Side effect profiles of psychedelics vary by drug class and the context in which they are used.
Serotonergic Psychedelics
Classic serotonergic psychedelics, including tryptamines and lysergamides (eg, psilocybin, LSD, mescaline, dimethyltryptamine [DMT], and 5-Methoxy-DMT), are generally well-tolerated in clinical and research settings across all age groups. However, their medical complications include headache, nausea, vomiting, dizziness, fatigue, and transient sympathomimetic effects.1–4 Typically, these AEs are dose dependent, transient, and resolve without the need for medical interventions. Serious AEs are rare in healthy individuals, but they can arise in those with cardiovascular conditions and in those who are taking other serotonergic agents, as this can raise the risk of seizures and serotonin syndrome.1–3 Psilocybin and its metabolite, psilocin, are both weak inhibitors of the human ether-a-go-go-related gene (hERG) potassium channel, which governs cardiac repolarization.2 While the doses required to produce clinically meaningful lengthening of the corrected QT (QTc) interval are significantly higher than those used in any clinical trial, individuals who are genetically predisposed to prolonged QT intervals—either due to genetic factors or to medication interactions—may be at increased risk.
Entactogens
Medical complications associated with the use of 3,4-methylenedioxymethamphetamine (MDMA) are primarily driven by its peripheral sympathetic effects and by metabolic dysregulation.5–7 MDMA’s most common medical AEs include transient tachycardia, hypertension, mydriasis, nystagmus, bruxism, headache, and sleep disturbances.5–7 Serious complications have been uncommon in clinical trials; however, arrhythmias and vascular events have occurred in those with underlying cardiovascular diseases.2,5 When hyperthermia develops, it can provoke a toxic cascade that results in rhabdomyolysis, disseminated intravascular coagulation, and/or subsequent acute liver and renal failure.5,6 MDMA-induced vasopressin release can provoke fluid retention and severe hyponatremia, which is further compounded by the intake of hypotonic fluids in unsupervised settings. The resulting electrolyte imbalance can lead to serious complications, eg, cerebral edema and seizures.5,6 Chronic use of high doses of MDMA has also been linked to reduced serotonin transporter density, suggesting the possibility of dose-dependent serotonin neurotoxicity in humans.7
Dissociative Anesthetics
Racemic ketamine and esketamine are the only legal and/or US Food and Drug Administration–approved psychedelic compounds, as studies of their use have generated more robust data compared to other psychedelics. Both agents demonstrate good tolerability with similar transient side effect profiles when used in accordance with clinical protocols.8,9 However, variability across compounds and routes of administration are linked to differences in pharmacokinetics and pharmacodynamics, which also impact the activity of metabolic byproducts (eg, norketamine and hydroxynorketamine).8,9 The most common medical AEs across all formulations of these agents include dizziness, nausea, vomiting, headache, and transient increases in blood pressure that typically resolve without a medical intervention.8,9 Serious cardiovascular events and stroke can occur secondary to acute hemodynamic effects; as a result, their clinical use is generally contraindicated in those with aneurysmal/hemorrhagic disease and cautioned in those with uncontrolled hypertension or elevated intraocular pressures. Ketamine can alter seizure threshold in a complex dose-dependent manner, and it can be proarrhythmic in individuals with underlying cardiovascular diseases.2,8 The risks of addiction and misuse potential are nontrivial due to its unique opioid receptor modulation, tolerance effects, and the lack of tachyphylaxis that is seen with classic psychedelics.8 This becomes particularly problematic if doses are escalated in recreational or at-home clinical settings, especially in the context of multiple substance use (as noted in case reports that have involved respiratory depression and death).8,9 Chronic or high-dose recreational use has also been linked to neurotoxic effects.9
Are Some Classes of Psychedelics More Medically Hazardous Than Others?
Two classes of psychedelics, the longer-acting substituted phenethylamines (a type of classic psychedelic) and ibogaine (an atypical psychedelic), deserve specific mention due to their increased risk of inducing medical AEs.
Other Substituted Phenethylamines
Most psychedelic phenethylamines show activity at 5-hydroxytryptamine 2A (5-HT2A) receptors, which conveys the theoretical risk of inducing a serotonin syndrome, with compound-specific risks associated with unique functional group substitutions.10–12 For example, 4-substituted-2,5-dimethoxyamphetamine (DOx) compounds are amphetamine derivatives of 2Cx compounds, and they are characterized by their extended duration of action and potent peripheral vasoconstrictive effects, which differentiate their risk profile from other substituted phenethylamines, such as MDMA.11,12 N-methoxybenzyl phenethylamine (NBOMe) compounds are known for their high potency at 5-HT2A receptors, and they have been associated with more severe toxicity and death. Although acute toxidromes from these 3 families of compounds have been poorly characterized in the medical literature, they often involve prolonged and severe hypertension and tachycardia with an increased theoretical risk posed to individuals with underlying cardiovascular diseases.11,12 Severe complications (eg, peripheral ischemia, rhabdomyolysis, and renal failure) associated with the use of DOx compounds due to the risk of potent and persistent vasoconstriction have been reported.11,12 Unlike DOx compounds, NBOMe agents have been linked to severe hyperthermia, metabolic acidosis, and multiorgan failure.11,12 To date, use of these agents has been largely limited to unsupervised recreational settings and observational or small, early-phase studies.10–12
Atypical Psychedelics
Ibogaine is a nonclassic psychedelic with a unique combination of mechanisms across multiple receptor classes, and its primary metabolite, noribogaine, persists for several days at clinically relevant concentrations, which contributes to its therapeutic and toxic potential.13,14 Acute AEs often involve intense nausea, vomiting, tremor, and ataxia. Ibogaine is associated with the highest documented risk for life-threatening cardiotoxicity among the psychedelics discussed above.13–15 The primary cardiac concern is for sudden cardiac death, as many fatalities have been reported after their use.2,13 Its cardiotoxicity is mediated by the potent blockade of the hERG potassium channel. Blockade of the hERG channel significantly delays ventricular repolarization, which results in dose-dependent QTc interval prolongation that increases the risk of polymorphic ventricular tachyarrhythmia, torsades de pointes.2,13,15 Postmortem and preclinical studies also suggest the potential for a dose-dependent cerebellar neurodegeneration that is mediated by its excitotoxic effects.13
What Physiological Changes and Drug Interactions Contribute to Medical Complications of Psychedelics?
Psychedelics produce a range of predictable physiological effects that vary by compound and receptor profile, forming the basis of many medical complications observed in both clinical and recreational settings. Classic serotonergic psychedelics (eg, psilocybin, LSD, mescaline) reliably produce transient autonomic activation (with increases in heart rate, blood pressure, and body temperature), related to a downstream release of epinephrine and cortisol.16,17 These changes are typically modest, self-limited, and well tolerated in healthy individuals; however, they may pose risks to those with uncontrolled hypertension, structural cardiac disease, or arrhythmias. In addition, nonspecific and less severe complications (eg, nausea, headaches, anxiety) of most psychedelics are typically dose dependent, occur within the acute dosing period, and resolve rapidly.18 These side effects may be related to serotonergic activation in the gastrointestinal (GI) tract (eg, nausea) and cerebral vasculature (eg, headache), occurring in similar frequency to the well-known side effects of nausea and headache from SSRI-induced serotonergic agonism.19,20
For clinical purposes, MDMA can mechanistically be thought of as a stimulant (eg, with reuptake inhibition of monoamines, such as dopamine, norepinephrine, and serotonin) with unique serotonergic properties (eg, direct release of serotonin, agonist at 5-HT2A receptors) like those of classic psychedelics. The levels of epinephrine released from classic psychedelics are similar to those of MDMA, although MDMA’s unique mechanism precipitates release of other monoamines, leading to more severe hyperthermia and a higher risk of other severe sympathomimetic toxicity, especially in recreational settings having a higher temperature, greater exertion, or poly-drug use.21 MDMA also inhibits cytochrome P450 (CYP) 2D6, which decreases its own clearance and increases the risk of nonlinear accumulation and drug-drug interactions with CYP2D6 substrates. These physiological and metabolic factors explain MDMA’s association with hyperthermia, rhabdomyolysis, hepatic injury, and, in rare cases, serotonin syndrome.22
Pharmacokinetic factors also contribute to adverse outcomes, particularly when psychedelics are combined with other medications. Psilocybin is a prodrug that is rapidly dephosphorylated to psilocin, which is metabolized through MAO-A, UGTs, and CYP isoenzymes.23 Concomitant use of monoamine oxidase inhibitors (MAOIs) may significantly increase psilocin exposure and intensify physiological and psychological effects.24 Strong CYP or UGT inhibitors may likewise prolong psilocin’s activity window. Unlike MAOIs, selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) may attenuate the effects of psychedelics rather than potentiate them, with no consistent evidence that these medications lead to an increased risk of serotonin syndrome and a general consensus that suggests that continuing these medications prior to clinical administration of psychedelics is safe and likely more tolerable than its discontinuation.25 Regarding psilocybin specifically, recent pharmacokinetic studies have demonstrated that psilocin exposure correlates nonlinearly with both peak subjective intensity and blood pressure elevation, suggesting that factors increasing psilocin area under the curve (AUC)—such as metabolic inhibition or delayed clearance—may disproportionately amplify adverse responses.23
Certain populations represent gaps in knowledge. No modern clinical trials have been conducted with adolescents, while older adults remain markedly underrepresented in studies, comprising only 1%–2% of trial participants,1,26 although a study of low-dose LSD in older adults failed to find an increased risk of impaired cognition or balance-related AEs.27 Specific risks in medically complex patients, such as those with cancer,28 remain poorly understood, and screening criteria for medical comorbidities vary widely across studies.
In sum, these physiological and pharmacologic mechanisms underscore the importance of comprehensive medical screening, medication review, and monitoring in both therapeutic and emergency care settings.
Can Chronic or High-Frequency Psychedelic Use Lead to Cumulative Toxicity?
Although there is no direct evidence that links classic psychedelics to valvular heart disease in humans, there is a theoretical risk of developing a cardiac valvulopathy associated with the frequent use and microdosing of classic psychedelics via 5-hydroxytryptamine receptor 2B (5-HT2B) receptor activity, the receptor implicated in phentermine-fenfluramine–induced valvulopathy.2,29 Classic psychedelics exert 5-HT2B partial agonism, which has raised concerns that long-term or high-frequency exposure could also cause valvular heart disease.30 Results of animal and clinical studies that have evaluated the risk of valvular heart disease with classic psychedelics have not been published, and we are unaware of case reports of valvular heart disease in users of classic psychedelics. Given the episodic nature of psychedelic use, including use in clinical trials assessing their therapeutic efficacy, it seems likely that valvular heart disease risk, if present, would be concentrated in individuals who use high doses at a high frequency. Outside of those with hallucinogen use disorder, the psychedelic users at highest risk would likely be those who “microdosed” psychedelics (eg, using a low-dose psychedelic every 3 days).31 Psychedelic science awaits epidemiologic and other data to determine whether classic psychedelics’ theoretical risk of valvular heart disease reflects a true clinical concern. In the meantime, patients using or considering using classic psychedelics, particularly if microdosing or engaging in other repetitive use, should be warned about this potential risk.
Although MDMA is not a potent direct 5-HT2B agonist, it substantially elevates extracellular serotonin by promoting release and inhibiting reuptake.32 In addition, its metabolite, (+/–)-3,4-methylenedioxyamphetamine (MDA), exhibits markedly greater 5-HT2B receptor agonist activity than MDMA itself.33 An in vitro study found that MDMA and MDA activate the 5-HT2B receptor at clinically relevant concentrations and stimulate proliferative signaling in human valvular interstitial cells in a manner like that induced by fenfluramine and its metabolite norfenfluramine in vivo.34 Unlike with classic psychedelics, case reports and observational data that document valvular heart disease in heavy MDMA users have been published.35,36 A small 2007 case-control study found that 28% of illicit MDMA users had abnormal echocardiographic findings consistent with valvulopathy, compared to none in matched controls.37 Importantly, the severity of valvulopathy was associated with cumulative MDMA exposure. Of note, this study recruited extremely heavy MDMA users, with the average MDMA-using subject reporting the use of 3.6 ± 6.7 MDMA tablets per week, with an average duration of use of 6.1 ± 3.4 years, potentially limiting its generalizability to occasional MDMA users or individuals receiving 1–3 doses in standard MDMA-assisted therapy clinical trial protocols. Despite the limitations of these data (particularly regarding their association with unusually high levels of MDMA use), individuals using or considering using MDMA should be warned about the potential risk for valvular heart disease with long-term MDMA use.
Ketamine, a drug for which we have a much greater evidence base than other psychedelics, appears to be well tolerated even with long-term use. Ulcerative cystitis and hepatobiliary inflammation are rare but have been observed with chronic and/or high-dose ketamine use, although this has not been observed in patients being treated with ketamine for psychiatric indications, despite chronic and repeated exposures occurring in depression clinics.11
How Should Clinicians Think About Long-Term Medical and Developmental Risks?
Classic psychedelics. Concerns that classic psychedelics, particularly LSD, might be carcinogenic or teratogenic emerged in the late 1960s after a study in Science found that adding high concentrations of LSD to cultured human leukocytes resulted in chromosomal abnormalities.38 Subsequently, reports suggested that the chromosomal changes seen mimicked patterns found in serious hematologic diseases. Some investigators described abnormalities that resembled the Philadelphia chromosome characteristic of chronic myeloid leukemia,39,40 while others noted alterations like those observed in Fanconi anemia and related cancer-prone syndromes.41 In addition, subsequent case reports linking nonmedical and medical LSD use to cancer, primarily leukemia, followed.42–47 Case reports and observational studies also suggested that LSD use during, or prior to, pregnancy could cause birth defects.
However, subsequent research has demonstrated that these fears were largely unfounded.48 Follow-up studies showed that the in vitro chromosomal abnormalities that were reported initially occurred in the setting of extremely high concentrations of LSD and for an unrealistic duration of exposure for humans.49 Their findings could not be reproduced at physiological doses, were no greater than those caused by common medications (eg, aspirin),50 and were confounded by polysubstance use, impure street LSD,51 and other factors, since subsequent studies found no long-lasting abnormalities in individuals who were treated with pharmaceutical-grade LSD.52–54 Some initial studies that suggested chromosomal damage resulted from LSD use were also retracted.55 Subsequent cytogenetic investigations in Indigenous communities (with long-standing ceremonial use of peyote56 and traditional hallucinogenic snuffs)57 were later shown to contain psychedelic compounds (eg, bufotenine and 5-MeO-DMT); they found no excess of chromosomal abnormalities in users compared with nonusers, which reinforced the view that classic psychedelics as a class do not carry meaningful chromosomal risk associated with carcinogenicity and germ line mutagenicity.
A review of this area by Cohen, who had fueled this controversy a decade earlier with the initial report38 of LSD’s effects on chromosomes, concluded that “LSD is not teratogenic. As to the drug’s oncogenic potential, the three reported cases of leukemia in LSD users are most likely the result of coincidence.”58 Contemporary epidemiologic studies of large numbers of psychedelic users have found no association between lifetime psychedelic use and either past year59 or lifetime cancer diagnoses.60
Regarding the use of classic psychedelics during pregnancy, rodent research with LSD has not found increased teratogenic risk following fetal exposure.61 Studies of zebrafish investigated fetal exposure to the classic psychedelics (eg, ayahuasca, DMT, LSD, mescaline, psilocybin, and psilocin).62 None of these induced morphological abnormalities in embryo-larvae. However, LSD was associated with locomotor impairments following developmental exposure. Ayahuasca was associated with edema and an increased mortality rate when used at high concentrations. Rodent studies have shown that ayahuasca enhances lethality to the embryo and the incidence of soft-tissue and skeleton anomalies in fetuses. However, the dosage that induced these effects was 4–8 times the dosage consumed by an average adult during an ayahuasca ritual ceremony.63 Data on ayahuasca use in pregnant women, as well as adolescent ayahuasca users (many who had been exposed in utero), are limited, although reassuring,64 with no suggestion of an increased risk of birth defects or neuropsychological impairments.65
While existing data for many psychedelics regarding teratogenic risk are reassuring, given the absence of large-scale human data and concerning findings from animal studies for some psychedelics (with the caveat that these are often associated with exposure to unusually high doses), it seems prudent for clinicians to counsel women to avoid use of classic psychedelics during pregnancy until stronger data that indicate safety are available.
MDMA. Two studies that investigated chronic adult exposure and developmental exposure in rats found that MDMA caused increased sperm DNA damage, although neither study demonstrated that the chromosomal breaks or micronucleus formation that define true germ-cell mutagenicity.66,67 Despite testicular changes and impaired sperm parameters, sperm morphology, fertility measures, and micronucleus testing were normal, suggesting that while MDMA produced genotoxic injury to sperm, it did not behave as a germ-line mutagen in rats. Reassuringly, a recent study that employed 3 in vitro test systems (Ames assay, chromosome aberration test, and micronucleus assay) found no evidence of MDMA-related genotoxicity (at or above clinically relevant concentrations), suggesting that there was no elevated carcinogenic or mutagenic risk.
Regarding teratogenic risks associated with fetal exposure, MDMA has not been shown to cause major structural malformations in animal models, but several studies have reported developmental neurotoxicity and adverse neurobehavioral outcomes. In rodents, prenatal and early postnatal MDMA exposure has led to impaired motor function, deficits in learning and memory, delayed physical and neurological development, and persistent neurochemical changes.68,69 Rodent studies have also identified concentration-dependent embryotoxicity.70 Human epidemiologic data have suggested that fetal exposure to MDMA is associated with delays in motor development and deficits in neuromotor functioning in infants up to 24 months of age, with a dose-dependent risk pattern.68,71 Given these data, women should be counseled to avoid MDMA during pregnancy.
Do Psychedelics Pose a Risk of Neurotoxicity or Cognitive Impairment?
Classic psychedelics. Concerns about potential adverse neurocognitive effects of classic psychedelics have persisted for decades. However, classic psychedelics fail to show a uniform pattern of neuropsychological impairment in controlled studies or in long-term observational cohorts.72 A cross-sectional observational study found that neuropsychological performance involving attention, memory, and visuospatial domains was broadly equivalent between sporadic classic psychedelic users and nonusers, with no evidence of cognitive harm.73 Modestly enhanced executive functioning, including superior performance on the Wisconsin Card Sorting Test (WCST), was demonstrated among psychedelic users. Dose-response analyses showed improved WCST performance with greater lifetime psychedelic exposure.
Survey data for individual classic psychedelics have shown that a randomized controlled trial of 89 healthy participants who were randomized to receive a single oral dose of 10 or 25 mg of psilocybin or placebo demonstrated no detrimental effects on global cognition, domain-specific functioning, or emotional processing at any time point up to 1 month after dosing.74 Multiple cross-sectional and longitudinal studies that compared long-term ayahuasca users with matched controls have found no evidence of cognitive decline or neuropsychological impairment, with some studies finding improved cognitive function, particularly in working memory and executive function.75–77 Comparable findings were found with long-term mescaline exposure. An observational study of Native American Church members who had ingested peyote hundreds to thousands of times over their lifetimes found no cognitive or psychological deficits compared to minimally exposed tribal controls.78 Importantly, within the peyote group, lifetime use did not correlate with neuropsychological performance. Unfortunately, modern studies that have investigated the cognitive effects of LSD are lacking; however, older studies of individuals exposed to LSD in nonmedical and medical settings showed no evidence of persistent neuropsychological deficits following exposure.79–81
MDMA. MDMA has been the subject of an extensive and controversial literature that linked heavy recreational use with serotonergic neurotoxicity and persistent neurocognitive deficits. Animal studies have consistently shown that high or repeated doses of MDMA can produce neurotoxicity associated with long-lasting serotonergic terminal loss, oxidative stress, mitochondrial dysfunction, inflammatory activation, and hyperthermia-mediated injury.7 However, the utility of interspecies scaling to predict human brain correlates from animal studies has been criticized due to significant differences between small animal and human brain metabolism of MDMA and enzymatic function.82,83 A primate study that purported to show dopaminergic neurotoxicity from MDMA was retracted after it was discovered that the primates had instead been administered methamphetamine.84 While the initial findings were widely reported in the media, news of the retraction was poorly disseminated.85
Human epidemiologic and neuropsychological studies have yielded more mixed results, but based on their findings, nonmedical MDMA use appears to be associated with mild to moderate, persistent, dose-dependent deficits in memory and, to a lesser extent, executive function and attention, with limited evidence for recovery after abstinence. Several earlier retrospective studies reported cognitive deficits (particularly in verbal memory, attention, and executive functioning) among MDMA users. However, most of these studies suffered from major confounding factors (including polydrug exposure, uncertain MDMA purity, and an inability to establish premorbid cognitive baselines). A Bradford Hill review found that the apparent association between MDMA and neurocognitive deficits often weakened or disappeared after accounting for these biases, with small meta-analytic effect sizes and inconsistent evidence of a dose-response relationship.86
Clinical trials of MDMA-assisted therapy have not produced published data on whether these findings extend to infrequent use of pharmaceutical grade MDMA in medical settings. Some of the most useful evidence for understanding nonmedical MDMA-specific adverse cognitive effects in humans arises from a study that examined unusually “pure” MDMA users with minimal exposure to other substances.87 That study of MDMA users matched with rave-involved MDMA-naive peers found that heavy MDMA users (with ≥60 lifetime uses) demonstrated statistically significant deficits in tasks that involved processing speed and impulsivity, while moderate users (with 22–50 uses) showed virtually no differences from controls. These results suggested a potential threshold and highlighted that MDMA-associated cognitive deficits were concentrated among individuals with high cumulative exposure. A recent meta-analysis found that MDMA users had worse learning and memory performance compared to MDMA-naive controls, with no significant difference between current and former MDMA users.88 Longer MDMA abstinence was not associated with smaller deficits in these areas compared to controls. Evidence of MDMA-associated neurocognitive impairment in other domains was more limited.
What Happened to Mr B?
Mr B was admitted to the intensive care unit and managed with aggressive supportive care, intravenous fluids, active cooling, and scheduled benzodiazepines. Over the following 24 hours, his vital signs stabilized, and his mental status improved. Once he was lucid, he confirmed that he had taken what he believed to be LSD purchased from a festival vendor. A friend who had purchased from the same source brought an additional tab to the hospital, which was sent for substance analysis. Confirmatory testing identified the compound as 25I-NBOMe, a potent synthetic psychedelic sometimes sold as LSD and associated with severe sympathomimetic and neurotoxic effects.
Mr B was monitored for an additional 48 hours and discharged with no residual neurologic deficits. He was counseled on the risks of novel psychoactive substances, particularly those misrepresented as classic psychedelics. His presentation was consistent with previously reported NBOMe intoxications. He was counseled on the risks of obtaining substances from unverified sources and received harm reduction education, including information about affordable reagent testing kits—such as those offered by DanceSafe—that can help detect the presence of NBOMe in products sold as LSD.
CONCLUSION
Medical complications from psychedelics, particularly those under the most intense research focus at present (psilocybin, LSD, MDMA, ketamine), are rare in clinical settings but may occur with higher frequency and severity with unsupervised use, particularly in the presence of polysubstance use, high doses, or underlying medical vulnerabilities. When individuals present for clinical evaluation with suspected psychedelic effects, medical assessment and management can generally be organized using familiar principles of supportive and toxidrome-based care, with prioritization of vital signs, temperature, hydration status, mental status, and identification of complications such as hyperthermia, electrolyte disturbance, or seizures, which typically declare themselves during the acute intoxication period. Once physiological stability and sensorium have returned, delayed or recrudescent medical sequelae are uncommon for most psychedelics, outside of atypical agents with known cardiotoxic or prolonged effects.
While some risks may have historically been exaggerated due to stigma, medical research on psychedelics is still in its infancy and much remains unknown, particularly on questions of longer-term use with frequent, high-dose exposures. Patients who may be seeking psychedelic treatments either licitly or illicitly, particularly those with known risk factors described above, should be counseled on these knowledge gaps.89 Clinicians should be prepared to offer evidence-informed guidance that neither minimizes known harms nor overstates unproven dangers, especially as interest in these substances continues to grow.
Article Information
Published Online: June 23, 2026. https://doi.org/10.4088/PCC.25f04171
© 2026 Physicians Postgraduate Press, Inc.
Submitted: December 18, 2025; accepted March 10, 2026.
To Cite: King F, Barnett BS, Taylor ST, et al. Medical complications of psychedelics. Prim Care Companion CNS Disord 2026;28(3):25f04171.
Author Affiliations: Center for Neuroscience of Psychedelics, Massachusetts General Hospital, Boston, Massachusetts (King); Department of Psychiatry, Harvard Medical School, Boston, Massachusetts (King, Taylor, Zambrano, Espi Forcen, Nigam, Stern); Cleveland Clinic Psychiatric Treatment Resistance Program, Cleveland Clinic, Cleveland, Ohio (Barnett); Home Base Massachusetts General Hospital, Boston, Massachusetts (Taylor); Neurotherapeutics Department, McLean Hospital, Boston, Massachusetts (Taylor); Department of Psychiatry, Massachusetts General/McLean Hospital, Boston, Massachusetts (Mattson, Zambrano, Nigam); Center for Neurointestinal Health, Department of Gastroenterology, Massachusetts General Hospital, Boston, Massachusetts (Mauney); Division of Pediatric Gastroenterology, Hepatology, and Nutrition, Tufts Medical Center, Boston, Massachusetts (Mauney); Lincoln Residence Program, McLean Hospital, Boston, Massachusetts (Espi Forcen).
Corresponding Author: Franklin King, IV, MD, Center for Neuroscience of Psychedelics, Massachusetts General Hospital, Boston, Massachusetts ([email protected]).
King, Barnett, Taylor, Mattson, and Mauney are co-first authors: Stern is the senior author.
Financial Disclosure: Dr King serves on the Scientific Advisory Board of Apex Labs, holds personal stock in Compass Pathways and Cybin, and has received research support from Tryp Therapeutics, the David Borsook Project, and the Tiny Blue Dot Foundation. Dr Barnett holds stock in Atai Lifesciences N.V. and CB Therapeutics (options); has served as an advisor for AbbVie, CB Therapeutics, Compass Pathways, GH Research, Livanova, Janssen, and MindMed; and receives monetary compensation for editorial work from DynaMed Plus (EBSCO Industries, Inc), speaker’s fees from TD Cowen, and research support from Abbott Laboratories, Compass Pathways, MindMed, and Reunion Neuroscience. Dr Mauney has received research support from Tryp Therapeutics. Dr Stern has received royalties from Elsevier for editing textbooks on Psychiatry. Drs Taylor, Mattson, Zambrano, Espi Forcen, and Nigam have no disclosures to report.
Clinical Points
- Classic serotonergic psychedelics (eg, psilocybin, lysergic acid diethylamide, mescaline) commonly cause transient elevations in blood pressure and heart rate, as well as nausea, dizziness, or headache; these effects are typically self-limited and clinically insignificant in healthy individuals.
- Although classic psychedelics produce 5-hydroxytryptamine receptor 2B5-HT2B agonism, the mechanism implicated in the development of Fen-Phen–induced cardiac valvulopathy. However, the clinical significance regarding psychedelics, particularly with longer-term use, remains unclear.
- 3,4-Methylenedioxymethamphetamine may provoke serious complications including hyperthermia, hyponatremia, rhabdomyolysis, and serotonin syndrome, particularly when used in hot environments or with excessive fluid intake. Repeated or high-dose use is associated with potential cardiac valvulopathy and possible neurocognitive changes.
- Ibogaine carries the highest known cardiotoxic risk among psychedelics due to corrected QT prolongation and risk of torsades de pointes, and it has been linked to sudden cardiac death in multiple case reports.
References (89)

- Hinkle JT, Graziosi M, Nayak SM, et al. Adverse events in studies of classic psychedelics: a systematic review and meta-analysis. JAMA Psychiatry. 2024;81(12):1225–1235. PubMed CrossRef
- Nahlawi A, Ptaszek LM, Ruskin JN. Cardiovascular effects and safety of classic psychedelics. Nat Cardiovasc Res. 2025;4(2):131–144. PubMed CrossRef
- Goodwin GM, Aaronson ST, Alvarez O, et al. Single-dose psilocybin for a treatment-resistant episode of major epression. N Engl J Med. 2022;387(18):1637–1648. CrossRef
- Robison R, Barrow R, Conant C, et al. Single treatment with MM120 (lysergide) in generalized anxiety disorder. JAMA. 2025;334(15):1358–1372. PubMed CrossRef
- Fonseca DA, Ribeiro DM, Tapadas M, et al. Ecstasy (3,4-methylenedioxymethamphetamine): cardiovascular effects and mechanisms. Eur J Pharmacol. 2021;903:174156. PubMed CrossRef
- Montgomery C, Roberts CA. Neurological and cognitive alterations induced by MDMA in humans. Exp Neurol. 2022;347:113888. PubMed CrossRef
- Costa G, Gołembiowska K. Neurotoxicity of MDMA: Main effects and mechanisms. Exp Neurol. 2022;347:113894. PubMed CrossRef
- Wan LB, Levitch CF, Perez AM, et al. Ketamine safety and tolerability in clinical trials for treatment-resistant depression. J Clin Psychiatry. 2014;76(03):247–252. PubMed CrossRef
- Li SW, Kumpf KT, Urrutia J, et al. Ketamine for depression, but at what cost? A review of ketamine’s neurotoxic effects from preclinical and human studies. Am J Psychiatry. 2025;182(10):903–912. CrossRef
- Schifano F, Chiappini S, Miuli A, et al. New psychoactive substances (NPS) and serotonin syndrome onset: a systematic review. Exp Neurol. 2021;339:113638. PubMed CrossRef
- Srisuma S, Bronstein AC, Hoyte CO. NBOMe and 2C substitute phenylethylamine exposures reported to the National Poison Data System. Clin Toxicol. 2015;53(7):624–628. PubMed CrossRef
- Zawilska JB, Kacela M, Adamowicz P. NBOMes–highly potent and toxic alternatives of LSD. Front Neurosci. 2020;14:78. PubMed CrossRef
- Litjens RPW, Brunt TM. How toxic is ibogaine?. Clin Toxicol. 2016;54(4):297–302. PubMed CrossRef
- Cherian KN, Keynan JN, Anker L, et al. Magnesium–ibogaine therapy in veterans with traumatic brain injuries. Nat Med. 2024;30(2):373–381. PubMed CrossRef
- Ona G, Rocha JM, Bouso JC, et al. The adverse events of ibogaine in humans: an updated systematic review of the literature (2015–2020). Psychopharmacology. 2022;239(6):1977–1987. PubMed CrossRef
- Schmid Y, Enzler F, Gasser P, et al. Acute effects of lysergic acid diethylamide in healthy subjects. Biol Psychiatry. 2015;78(8):544–553. CrossRef
- Vollenweider FX, Kometer M. The neurobiology of psychedelic drugs: implications for the treatment of mood disorders. Nat Rev Neurosci. 2010;11(9):642–651. PubMed CrossRef
- Yerubandi A, Thomas JE, Bhuiya NMMA, et al. Acute adverse effects of therapeutic doses of psilocybin. JAMA Netw Open. 2024;7(4):e245960. CrossRef
- Carhart-Harris R, Giribaldi B, Watts R, et al. Trial of psilocybin versus escitalopram for depression. N Engl J Med. 2021;384(15):1402–1411. CrossRef
- Johnson MW, Sewell RA, Griffiths RR. Psilocybin dose-dependently causes delayed, transient headaches in healthy volunteers. Drug Alcohol Depend. 2012;123(1-3):132–140. PubMed CrossRef
- Hysek CM, Simmler LD, Ineichen M, et al. The norepinephrine transporter inhibitor reboxetine reduces stimulant effects of MDMA (“ecstasy”) in humans. Clin Pharmacol Ther. 2011;90(2):246–255. PubMed CrossRef
- Yang J, Jamei M, Heydari A, et al. Implications of mechanism-based inhibition of CYP2D6 for the pharmacokinetics and toxicity of MDMA. J Psychopharmacol. 2006;20(6):842–849. PubMed CrossRef
- Brown RT, Nicholas CR, Cozzi NV, et al. Pharmacokinetics of escalating doses of oral psilocybin in healthy adults. Clin Pharmacokinet. 2017;56(12):1543–1554. PubMed CrossRef
- Malcolm B, Thomas K. Serotonin toxicity of serotonergic psychedelics. Psychopharmacology. 2022;239(6):1881–1891. PubMed CrossRef
- Tap SC, Thomas K, Páleníček T, et al. Concomitant use of antidepressants and classic psychedelics: a scoping review. J Psychopharmacol. 2025;39(10):1072–1088. PubMed CrossRef
- Bouchet L, Sager Z, Yrondi A, et al. Older adults in psychedelic-assisted therapy trials: a systematic review. J Psychopharmacol. 2024;38(1):33–48. PubMed CrossRef
- Family N, Maillet EL, Williams LTJ, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of low dose lysergic acid diethylamide (LSD) in healthy older volunteers. Psychopharmacology. 2020;237(3):841–853. PubMed CrossRef
- Beaussant Y, Sager Z, Brennan C, et al. Psilocybin-assisted therapy for demoralisation in hospice patients: feasibility, safety and preliminary efficacy. BMJ Support Palliat Care. 2025. spcare-2025-005773.
- Hutcheson JD, Setola V, Roth BL, et al. Serotonin receptors and heart valve disease-it was meant 2B. Pharmacol Ther. 2011;132(2):146–157. PubMed CrossRef
- Tagen M, Mantuani D, Heerden L, et al. The risk of chronic psychedelic and MDMA microdosing for valvular heart disease. J Psychopharmacol. 2023;37(9):876–890. PubMed CrossRef
- Polito V, Stevenson RJ. A systematic study of microdosing psychedelics. PLoS ONE. 2019;14(2):e0211023. PubMed CrossRef
- McIntyre RS. Serotonin 5-HT2B receptor agonism and valvular heart disease: implications for the development of psilocybin and related agents. Expert Opin Drug Saf. 2023;22(10):881–883. CrossRef
- Luethi D, Kolaczynska KE, Walter M, et al. Metabolites of the ring-substituted stimulants MDMA, methylone and MDPV differentially affect human monoaminergic systems. J Psychopharmacol (Oxf, Engl). 2019;33(7):831-841. PubMed CrossRef
- Setola V, Hufeisen SJ, Grande-Allen KJ, et al. 3,4-Methylenedioxymethamphetamine (MDMA, “Ecstasy”) induces fenfluramine-like proliferative actions on human cardiac valvular interstitial cells in vitro. Mol Pharmacol. 2003;63(6):1223–1229. PubMed CrossRef
- Sol B, Nijs J, Forsyth R, et al. Methylenedioxymethamphetamine-induced toxic valvulopathy. Eur Hear J Case Rep. 2020;4(6):1–2. PubMed CrossRef
- Montastruc F, Montastruc G, Vigreux P, et al. Valvular heart disease in a patient taking 3,4-methylenedioxymethamphetamine (MDMA, ‘Ecstasy’). Br J Clin Pharmacol. 2012;74(3):547–548. PubMed CrossRef
- Droogmans S, Cosyns B, D’haenen H, et al. Possible association between 3,4-methylenedioxymethamphetamine abuse and valvular heart disease. Am J Cardiol. 2007;100(9):1442–1445. PubMed CrossRef
- Cohen MM, Marinello MJ, Back N. Chromosomal damage in human leukocytes induced by lysergic acid diethylamide. Science. 1967;155(3768):1417–1419. PubMed CrossRef
- Egozcue J, Irwin S, Maruffo CA. Chromosomal damage in LSD users. JAMA. 1968;204(3):214–218. PubMed CrossRef
- Irwin S, Egozcue J. Chromosomal abnormalities in leukocytes from LSD-25 users. Science. 1967;157(3786):313–314. PubMed CrossRef
- Cohen MM, Hirschhorn K, Frosch WA. In vivo and in vitro chromosomal damage induced by LSD-25. N Engl J Med. 1967;277(20):1043–1049. PubMed CrossRef
- Berliner AD, Distenfeld A. Hodgkin’s disease in a married couple. JAMA. 1972;221(7):703–704. PubMed
- Goh K, Bauman AW. Lysergic acid diethylamide and acute leukemia. J Am Med Women’s Assoc (1972). 1978;33(10):419–422. PubMed
- Grossbard L, Rosen D, McGilvray E, et al. Acute leukemia with Ph1-like chromosome in an LSD user. JAMA. 1968;205(11):791–793. PubMed
- Levick LJ, Levick SN. Testicular choriocarcinoma in LSD users: coincidence or cause?. JAMA. 1971;217(4):475–476. PubMed
- Sohn K, Boggs DR. Klinefelter’s syndrome, LSD usage and acute lymphoblastic leukemia. Clin Genet. 1974;6(1):20–22. PubMed CrossRef
- Garson OM, Robson MK. Studies in a patient with acute leukaemia after lysergide Treatment. Br Med J. 1969;2(5660):800. PubMed CrossRef
- Houston BK. Review of the evidence and qualifications regarding the effects of hallucinogenic drugs on chromosomes and embryos. Am J Psychiatry. 1969;126(2):251–254. PubMed CrossRef
- Dishotsky NI, Loughman WD, Mogar RE, et al. LSD and genetic damage. Science. 1971;172(3982):431–440. PubMed CrossRef
- Kato T, Jarvik LF. LSD-25 and genetic damage. Dis Nerv Syst. 1969;30(1):42–46. PubMed
- Grof S. LSD Psychotherapy. 1st ed.. Hunter House; 1980.
- Corey MJ, Andrews JC, McLeod MJ, et al. Chromosome studies on patients (in vivo) and cells (in vitro) treated with lysergic acid diethylamide. N Engl J Med. 1970;282(17):939–943. PubMed CrossRef
- Hungerford DA, Taylor KM, Shagass C, et al. Cytogenetic effects of LSD 25 therapy in man. JAMA. 1968;206(10):2287–2291. PubMed
- Jarvik LF, Yen FS, Dahlberg CC, et al. Chromosome examinations after medically administered lysergic acid diethylamide and dextroamphetamine. Dis Nerv Syst. 1974;35(9):399–407. PubMed
- Schlag AK, Aday J, Salam I, et al. Adverse effects of psychedelics: from anecdotes and misinformation to systematic science. J Psychopharmacol. 2022;36(3):258–272. PubMed CrossRef
- Dorrance DL, Janiger O, Teplitz RL. Effect of peyote on human chromosomes: cytogenetic study of the Huichol Indians of Northern Mexico. JAMA. 1975;234(3):299–302. PubMed
- Bloom AD, Neel JV, Choi KW, et al. Chromosome aberrations among the Yanomamma Indians. Proc Natl Acad Sci United States Am. 1970;66(3):920–927. PubMed CrossRef
- Cohen MM, Shiloh Y. Genetic toxicology of lysergic acid diethylamide (LSD-25). Mutat Res. 1978;47(3-4):183–209. PubMed CrossRef
- Simonsson O, Sexton JD, Hendricks PS. Associations between lifetime classic psychedelic use and markers of physical health. J Psychopharmacol Oxf, Engl. 2021;35(4):447–452. PubMed CrossRef
- Barnett BS, Ziegler K, Doblin R, et al. Is psychedelic use associated with cancer?: Interrogating a half-century-old claim using contemporary population-level data. J Psychopharmacol. 2022;36(10):1118–1128. PubMed CrossRef
- Warkany J, Takacs E. Lysergic acid diethylamide (LSD): No teratogenicity in rats. Science. 1968;159(3816):731–732. PubMed CrossRef
- Oliveira ALde, Oliveira DPde, Santos RG, et al. Psychedelic-induced behavioral and developmental effects on zebrafish: a systematic review. Prog Neuro-Psychopharmacol Biol Psychiatry. 2025;142:111534.
- Motta LGda, Morais JAde, Tavares ACAM, et al. Maternal and developmental toxicity of the hallucinogenic plant-based beverage ayahuasca in rats. Reprod Toxicol. 2018;77:143–153. PubMed CrossRef
- Labate BC. Consumption of ayahuasca by children and pregnant women: medical controversies and religious perspectives. J Psychoact Drugs. 2011;43(1):27–35. PubMed CrossRef
- Doering-Silveira E, Lopez E, Grob CS, et al. Ayahuasca in adolescence: neuropsychological assessment. J Psychoact Drugs. 2005;37(2):123–128. PubMed CrossRef
- Barenys M, Macia N, Camps L, et al. Chronic exposure to MDMA (ecstasy) increases DNA damage in sperm and alters testes histopathology in male rats. Toxicol Lett. 2009;191(1):40–46. PubMed CrossRef
- Barenys M, Gomez-Catalan J, Camps L, et al. MDMA (ecstasy) delays pubertal development and alters sperm quality after developmental exposure in the rat. Toxicol Lett. 2010;197(2):135–142. PubMed CrossRef
- Barenys M, Reverte I, Masjosthusmann S, et al. Developmental neurotoxicity of MDMA. A systematic literature review summarized in a putative adverse outcome pathway. NeuroToxicology. 2020;78:209–241. PubMed CrossRef
- Skelton MR, Williams MT, Vorhees CV. Developmental effects of 3,4-methylenedioxymethamphetamine: a review. Behav Pharmacol. 2008;19(2):91–111. PubMed CrossRef
- Barenys M, Flick B, Boix N, et al. Effects of MDMA (ecstasy) and two of its metabolites on rat embryos in vitro. Reprod Toxicol. 2012;34(1):57–65. PubMed CrossRef
- Singer LT, Moore DG, Min MO, et al. Motor delays in MDMA (ecstasy) exposed infants persist to 2 years. Neurotoxicol Teratol. 2016;54:22–28. PubMed CrossRef
- Basedow LA, Riemer TG, Reiche S, et al. Neuropsychological functioning in users of serotonergic psychedelics – a systematic review and meta-analysis. Front Pharmacol. 2021;12:739966. PubMed CrossRef
- Reiche S, Hirschfeld T, Gröticke AL, et al. Sporadic use of classic psychedelics and neuropsychological performance: a cross-sectional analysis. Prog Neuro-Psychopharmacol Biol Psychiatry. 2025;138:111353. PubMed CrossRef
- Rucker JJ, Marwood L, Ajantaival RLJ, et al. The effects of psilocybin on cognitive and emotional functions in healthy participants: results from a phase 1, randomised, placebo-controlled trial involving simultaneous psilocybin administration and preparation. J Psychopharmacol Oxf, Engl. 2022;36(1):114–125. PubMed CrossRef
- Fonseca AM, Santos RG, Medeiros LS, et al. Long-term ayahuasca use is associated with preserved global cognitive function and improved memory: a cross-sectional study with ritual users. Eur Arch Psychiatry Clin Neurosci. 2025;275(2):519–531. PubMed CrossRef
- Bouso JC, González D, Fondevila S, et al. Personality, psychopathology, life attitudes and neuropsychological performance among ritual users of ayahuasca: longitudinal study. PLoS ONE. 2012;7(8):e42421. PubMed CrossRef
- Barbosa PCR, Strassman RJ, Silveira DX, et al. Psychological and neuropsychological assessment of regular hoasca users. Compr Psychiatry. 2016;71:95–105. PubMed CrossRef
- Halpern JH, Sherwood AR, Hudson JI, et al. Psychological and cognitive effects of long-term peyote use among Native Americans. Biol Psychiatry. 2005;58(8):624–631. PubMed CrossRef
- Wright M, Hogan TP. Repeated LSD ingestion and performance on neuropsychological tests. J Nerv Ment Dis. 1972;154(6):432–438. PubMed CrossRef
- McGlothlin WH, Arnold DO, Freedman DX. Organicity measures following repeated LSD ingestion. Arch Gen Psychiatry. 1969;21(6):704–709. PubMed CrossRef
- Basedow LA, Riemer TG. Acute effects and long-term neuropsychological consequences of classic psychedelics use. Curr Top Behav Neurosci. 2025:1–18.
- Vollenweider FX, Jones RT, Baggott MJ. Caveat emptor: editors beware. Neuropsychopharmacology. 2001;24(4):461–463. PubMed CrossRef
- Torre R, Farré M. Neurotoxicity of MDMA (ecstasy): the limitations of scaling from animals to humans. Trends Pharmacol Sci. 2004;25(10):505–508. PubMed CrossRef
- Ricaurte GA, Yuan J, Hatzidimitriou G, et al. Severe dopaminergic neurotoxicity in primates after a common recreational dose regimen of MDMA (“Ecstasy”). Science. 2002;297(5590):2260–2263. PubMed CrossRef
- Barnett BS, Doblin R. Dissemination of erroneous research findings and subsequent retraction in high-circulation newspapers: a case study of alleged MDMA-induced dopaminergic neurotoxicity in primates. J Psychoact Drugs. 2021;53(2):104–110. PubMed CrossRef
- Amoroso T. The spurious relationship between ecstasy use and neurocognitive deficits: a Bradford Hill review. Int J Drug Polic. 2019;64:47–53. PubMed CrossRef
- Halpern JH, Pope HG, Sherwood AR, et al. Residual neuropsychological effects of illicit 3,4-methylenedioxymethamphetamine (MDMA) in individuals with minimal exposure to other drugs. Drug Alcohol Depend. 2004;75(2):135–147. PubMed CrossRef
- Ung H, McKeon G, Jokovic Z, et al. Long-term neurocognitive side effects of MDMA in recreational ecstasy users following sustained abstinence: a systematic review and meta-analysis. J Psychopharmacol. 2025:2698811251389559.
- King F, Nahlawi A, Stern TA. Talking to your patients about psychedelics: using an informed approach and understanding indications, risks, and benefits. Prim Care Companion CNS Disord. 2024;26(5):24f03783. PubMed CrossRef
Please sign in or purchase this PDF for $40.




